Introduction
If you work with metabolic disorders, cardiovascular health, or clinical nutrition, you already know that hypertension is rarely just a “blood pressure problem.” It is a regulatory problem.
Yet in everyday practice even among trained professionals hypertension classification is often reduced to a simple binary: primary vs secondary. Useful? Yes. Sufficient? Not even close.
Understanding the types of hypertension is not merely an academic exercise. It fundamentally changes how you investigate root causes, interpret clinical data, and design interventions that actually modify physiology rather than temporarily suppress numbers.
For many practitioners, the real challenge is this:
You see elevated blood pressure.
You see metabolic dysfunction.
You see nervous system dysregulation.
But how do you know whether these are drivers, adaptations, or consequences?
That distinction begins with understanding the difference between essential hypertension and secondary hypertension, and not just definitionally, but mechanistically.
This article will help you interpret hypertension classification through a regulatory systems model involving:
- neurovascular control
- metabolic signaling
- renal regulation
- endocrine modulation
- structural vascular adaptation
Because blood pressure is never controlled by one organ. It is controlled by communication between systems.
Hypertension as a Regulatory Failure, Not a Pressure Disorder
Before discussing classification, you must first reframe the physiology.
Blood pressure exists to maintain perfusion stability.
It is an output of regulation, and not an independent variable.
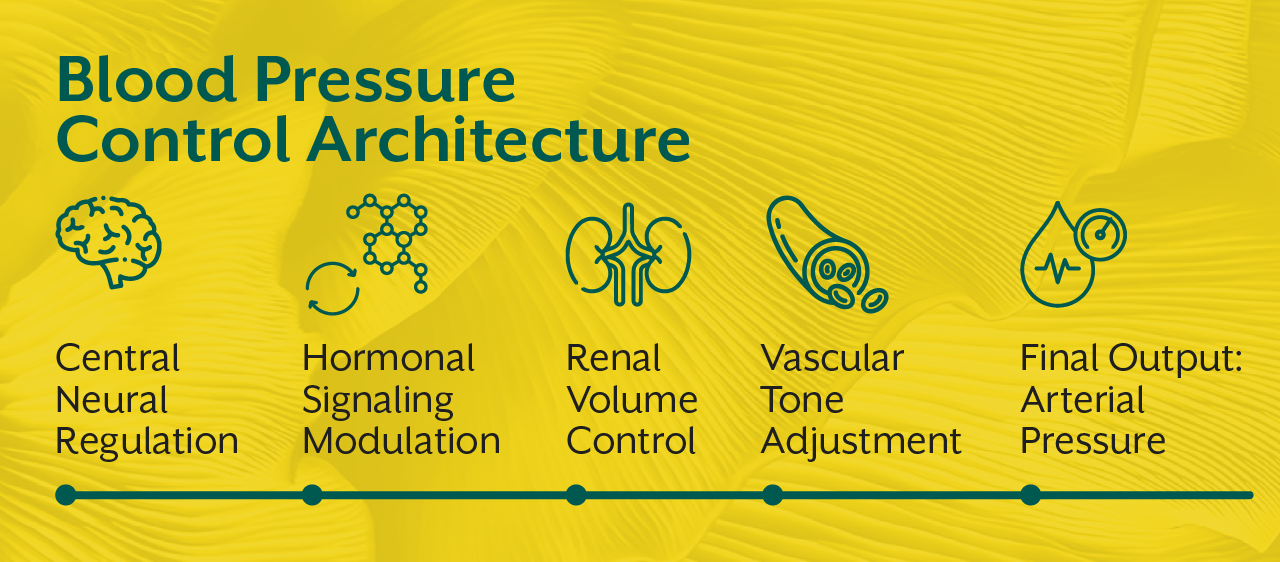
Three major control networks constantly negotiate pressure:
- Neural control – autonomic tone, baroreflex responsiveness
- Volume control – renal sodium handling, plasma expansion
- Vascular tone control – endothelial signaling, smooth muscle response
Hypertension develops when regulatory calibration shifts upward and stabilizes at a new set point.
The key clinical question becomes:
What reset the system?
That answer determines whether hypertension is classified as essential or secondary.
What Is Essential Hypertension? A Network Disorder Without a Single Trigger
Essential hypertension accounts for nearly 90–95% of clinical cases. Traditionally, it is defined as hypertension without an identifiable medical cause.
But this definition is incomplete.
Essential hypertension is not “without cause.”
It is without a single dominant cause.
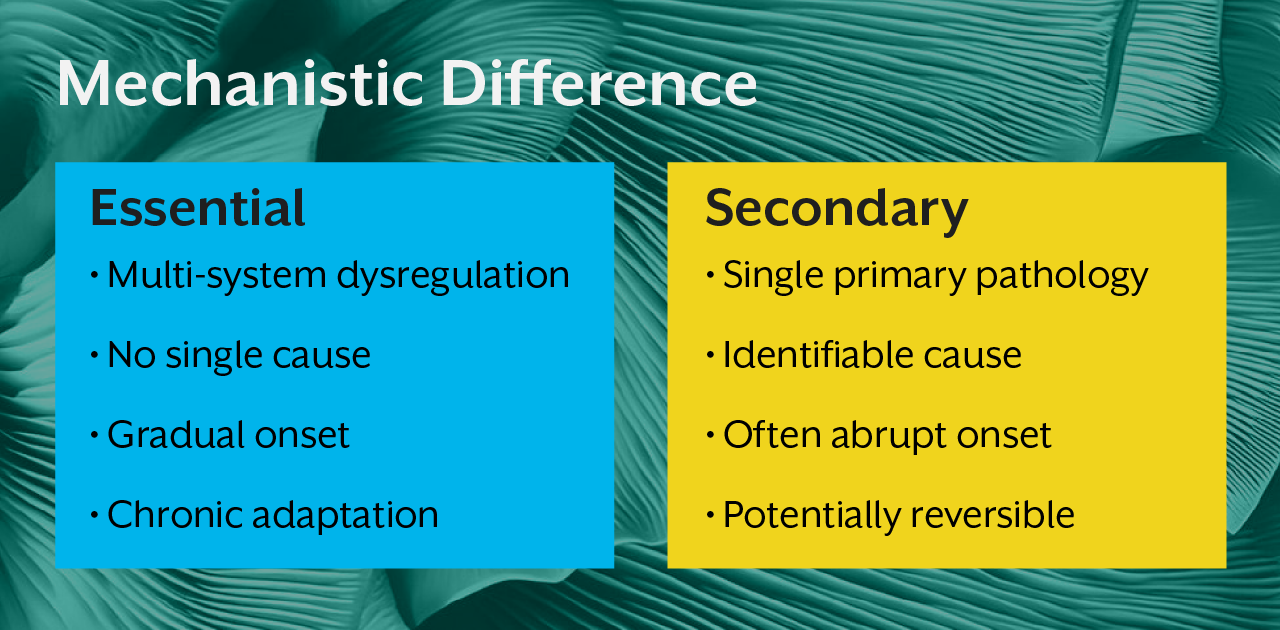
It emerges from long-term regulatory recalibration across multiple systems. No single pathology explains it but system interactions do.
Core mechanisms involved
1. Autonomic imbalance
Persistent sympathetic dominance increases vascular resistance and cardiac output. Reduced vagal buffering impairs pressure stabilization.
2. Endothelial signaling dysfunction
Nitric oxide production declines. Vascular smooth muscle responsiveness increases. Structural remodeling begins.
3. Renal pressure-natriuresis shift
The kidneys require higher pressure to excrete sodium effectively. Volume regulation becomes pressure-dependent.
4. Metabolic signaling impairment
Insulin resistance, adipokine signaling, and mitochondrial inefficiency alter vascular responsiveness and sodium retention.
5. Central regulatory reset
Hypothalamic control of cardiovascular tone recalibrates in response to chronic environmental and metabolic signals.
This is why essential hypertension progresses gradually and stabilizes chronically. The system has adapted to a new equilibrium.

Nervous System Dominance - The Most Under-Recognized Driver
Practitioners often focus on vascular resistance and renal function. But long-term pressure set-point is strongly governed by central autonomic control.
Chronic sympathetic activation does three powerful things:
- raises baseline vascular tone
- increases renal sodium retention
- promotes vascular structural remodeling
Over time, baroreceptors adapt to higher pressure ranges. What was once hypertensive becomes physiologically “normal” to the brainstem.
This is why stress physiology, sleep disruption, metabolic signaling, and inflammation all converge in essential hypertension. They all influence autonomic calibration.
If you are treating numbers without restoring regulatory variability, you are managing output without correcting control architecture.
This system's perspective is explored further in the iThrive Academy blog “Decoding Functional Sports Nutrition: How Electrolytes and HRV Define True Athletic Recovery,” which explains how nervous system balance determines cardiovascular recovery efficiency, the same principle governing long-term blood pressure regulation.
What Is Secondary Hypertension? A Pressure Response to a Specific Pathology
Secondary hypertension differs fundamentally from essential hypertension.
It is not a network adaptation.
It is a physiological response to an identifiable primary disorder.
The regulatory system itself may be functioning correctly but responding to abnormal inputs.
Common causes include:
- renal artery stenosis
- chronic kidney disease
- endocrine hormone excess
- medication effects
- structural vascular abnormalities
Here, elevated pressure is compensatory or driven by a defined pathological signal.
Remove the cause → pressure normalizes.
That reversibility is the defining feature.
The Endocrine Dimension of Secondary Hypertension
Some of the most clinically significant secondary forms arise from endocrine dysregulation.
Hormones that strongly influence pressure include:
- aldosterone (sodium retention)
- cortisol (vascular sensitivity amplification)
- catecholamines (sympathetic overactivation)
- thyroid hormones (cardiac output modulation)
In endocrine-driven hypertension, pressure rises because signaling intensity changes, not because regulatory architecture fails.
Understanding hormonal signaling hierarchies is essential for accurate diagnosis. This integrative endocrine-metabolic framework is also discussed in the iThrive Academy article “Insulin Resistance: The Silent Phase Before Type 2 Diabetes,” which demonstrates how endocrine signaling disruptions precede overt disease expression.
Structural vs Functional Hypertension - A Clinical Interpretation Layer
Another useful practitioner lens is structural versus functional pressure elevation.
Essential hypertension begins as functional dysregulation but gradually induces structural vascular remodeling in the form of arterial stiffness, smooth muscle hypertrophy, reduced compliance.
Secondary hypertension may arise from structural abnormalities first, with functional responses following.
Recognizing which came first helps guide intervention strategy.
Why Classification Matters for Practitioners and Learners
If you are building a clinical career, this distinction affects everything:
- diagnostic testing strategy
- interpretation of biomarkers
- intervention hierarchy
- long-term prognosis
- reversibility expectations
Many practitioners struggle because patients rarely present with purely essential or purely secondary patterns. Mixed physiology is common.
This is where systems-level training becomes critical, the ability to interpret interactions rather than isolated findings.
Programs like those offered by iThrive Academy train practitioners to read regulatory physiology across organ systems, not just disease labels. Within the iThrive Certified Functional Nutrition (ICFN) framework, hypertension is studied through metabolic, neuroregulatory, and endocrine integration, the level required for true root-cause clinical work.
Hypertension Classification Is a Continuum, Not a Binary
In real physiology, essential and secondary hypertension are conceptual anchors, and not rigid categories.
A patient may begin with endocrine-driven pressure elevation.
Chronic exposure then remodels vascular structure.
Autonomic tone resets.
What began as secondary evolves into essential.
Conversely, long-standing essential hypertension can produce renal damage, eventually creating secondary components later.
Understanding this bidirectional evolution is what differentiates algorithm-based management from true clinical reasoning.
Key Takeaway
The distinction between essential hypertension and secondary hypertension is not merely diagnostic labeling, it reflects fundamentally different regulatory dynamics. Essential hypertension represents a distributed systems recalibration driven by chronic neural, metabolic, vascular, and renal signaling shifts. Secondary hypertension, in contrast, is a pressure response to a specific pathological driver that disrupts otherwise functional regulatory mechanisms.
For practitioners, the real clinical skill lies in identifying where on this spectrum a patient lies, how regulatory networks have adapted over time, and whether pressure elevation is compensatory, structural, or centrally programmed. Only when hypertension is understood as a systems-level control problem rather than a single-organ disorder, creative meaningful, lasting interventions be designed.




.jpg)