Introduction
Every week, millions of women walk into clinics across India describing the same constellation of symptoms. Fatigue that no amount of sleep fixes. Weight that refuses to shift despite disciplined eating. Moods that swing unpredictably. Periods that are painful, irregular, or simply wrong. Skin that breaks out like a teenager's. And a nagging sense that something deeper is going on.
What do most of them hear? "Your labs are normal." Or they leave with oral contraceptives, an antidepressant, or a thyroid medication, each targeting one isolated symptom while the root cause quietly multiplies downstream.
This highlights a key limitation in conventional approaches when it comes to understanding hormonal imbalance in women. It treats individual hormones like isolated departments, never reading the internal memo that says they all work in the same building.
If you are a practitioner trying to genuinely help female patients, or if you are a woman navigating this yourself, what follows is a functional lens that may offer a more comprehensive perspective.
What Actually Causes Hormonal Imbalance in Women?
Hormonal imbalance in women is not a single condition. It is a system failure, and the causes are rarely singular.
The most common drivers include chronic psychological and physiological stress, nutrient depletion, poor sleep, environmental toxin exposure, gut dysbiosis, insulin resistance, and impaired liver detoxification. These factors do not operate independently. They feed each other in loops that conventional lab panels, ordered one hormone at a time, are simply not designed to catch.
At the core of female hormone health sit estrogen, progesterone, cortisol, thyroid hormones, and insulin. When any one of these begins to dysregulate, the ripple effect through the others is significant and predictable. Understanding those ripples is exactly what separates a functional approach from a pharmaceutical one.
Estrogen Dominance: The Most Misunderstood Hormonal Pattern
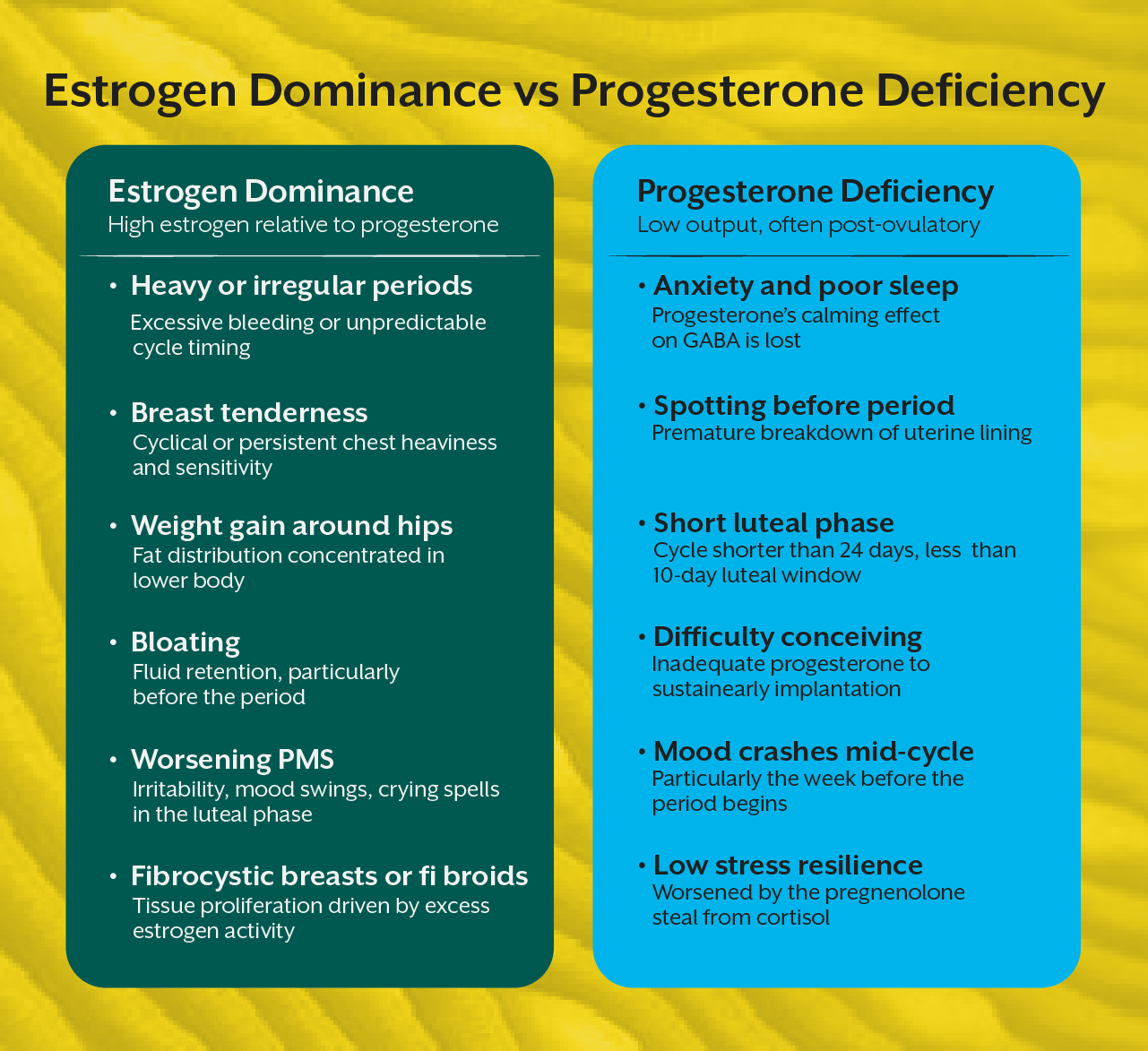
Estrogen dominance does not always mean a woman has too much estrogen. It means estrogen is high relative to progesterone, and the consequences are felt regardless of whether absolute estrogen levels sit within the standard reference range on a blood test.
Signs of estrogen dominance include heavy or irregular periods, breast tenderness, bloating, mood instability, difficulty losing weight particularly around the hips and thighs, and worsening PMS. Many women living with this pattern have been told their hormones are "fine" because their estrogen level, viewed alone, did not trigger a flag.
The functional investigation looks further. It examines how estrogen is being metabolised, specifically which liver detoxification pathways are handling it. The 2:16 hydroxylation ratio, measured through DUTCH testing or urinary hormone metabolite panels, reveals whether estrogen is clearing through protective pathways or being shunted toward more proliferative metabolites. It also looks at whether the gut is reabsorbing already conjugated estrogen due to an overactive beta glucuronidase enzyme, a product of certain bacterial strains. This is the estrobolome, the subset of gut microbiota responsible for estrogen metabolism, and it is almost entirely absent from conventional endocrine workups.
Nutritionally, estrogen dominance can often improve with targeted intervention. Cruciferous vegetables supply indole 3 carbinol and DIM, which support safer hydroxylation pathways. Adequate dietary fibre supports estrogen excretion. Addressing dysbiosis reduces enterohepatic recirculation. Liver support through nutrients like N acetyl cysteine, sulforaphane, and B vitamins keeps phase two detoxification running.
Progesterone Deficiency: The Quiet Epidemic
If estrogen dominance is over-represented in clinical conversation, progesterone deficiency is drastically under-discussed. And yet, low progesterone is extraordinarily common in women between 25 and 45, the demographic carrying the highest allostatic load of stress, career pressure, and reproductive demands.
Progesterone is produced primarily after ovulation. This means anovulatory cycles, which can occur without obvious symptoms, quietly eliminate progesterone production for that entire month. Under chronic stress, the body preferentially shuttles the progesterone precursor pregnenolone toward cortisol synthesis. This is the pregnenolone steal, and it is a direct pathway by which psychological stress creates progesterone deficiency signs: anxiety, sleep disruption, spotting before periods, shortening luteal phases, and infertility.
Standard blood tests measuring progesterone on day 21 of a cycle catch only a narrow window. DUTCH testing across multiple cycle points provides a far more complete picture of progesterone output and its metabolites.
Supporting progesterone production naturally often involves addressing adrenal burden as a key factor. If cortisol demand remains high, nutrient interventions alone may have limited impact.
The Cortisol and Sex Hormone Connection That Conventional Medicine Ignores
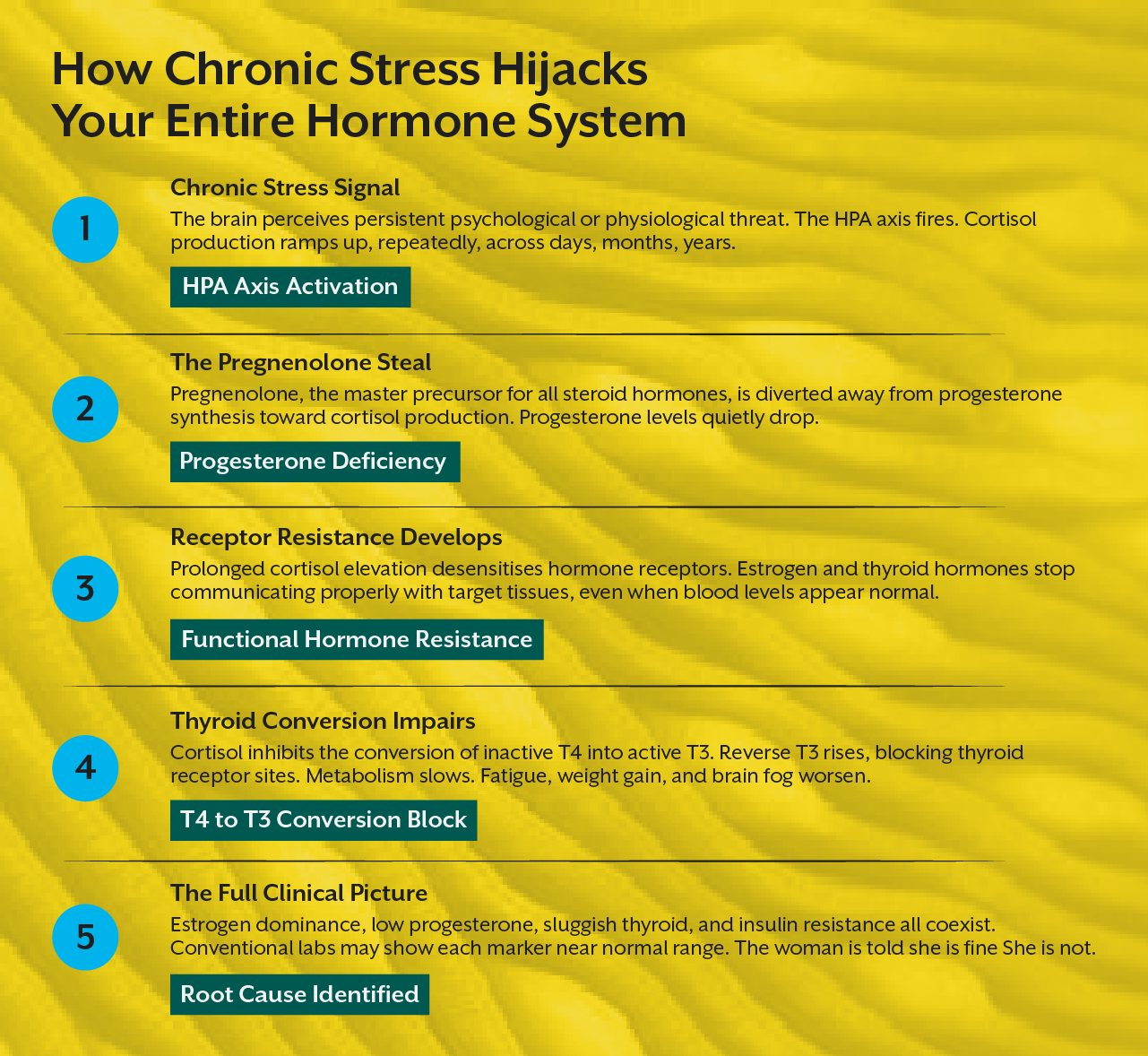
Cortisol is not just a stress hormone. It is a master regulator that communicates directly with reproductive hormones, the thyroid, blood sugar systems, and immune function.
When cortisol is chronically elevated, which in modern Indian urban life is not the exception but the norm, several things happen simultaneously. Progesterone is depleted via the pregnenolone pathway. The sensitivity of hormone receptors decreases, meaning even adequate estrogen and thyroid hormone fail to generate a proper cellular response. Insulin sensitivity worsens. And because cortisol and sex hormones compete for the same feedback loops in the hypothalamic pituitary axis, the brain's signalling to the ovaries becomes dysregulated at the source.
This is why addressing adrenal function is an important part of managing hormonal imbalance in women.
Functional lab markers include a four point salivary or urinary cortisol curve, DHEA S, and morning cortisol to DHEA ratios. Nutritional support centres on adaptogenic herbs like ashwagandha and rhodiola, magnesium glycinate, and phosphatidylserine, alongside removing the lifestyle inputs sustaining the threat response.
The Thyroid Connection: Why Thyroid Hormone Disorders in Women Are Chronically Under-Diagnosed
The thyroid gland is profoundly sensitive to the same stressors that disrupt sex hormones. Chronic stress reduces conversion of T4 to active T3. Estrogen dominance raises thyroid binding globulin, reducing free thyroid hormone availability. Nutrient deficiencies in selenium, iodine, zinc, and iron impair both synthesis and conversion.
Yet a standard thyroid panel in most clinics measures only TSH. Sometimes T4 is included. Rarely are free T3, reverse T3, or thyroid antibodies assessed unless the TSH is already out of range. This is a problem because a woman can have optimal TSH, suboptimal free T3, elevated reverse T3, and early autoimmune thyroid activity all at once, and her panel will be reported as normal.
Symptoms of suboptimal thyroid function overlap substantially with general hormonal imbalance in women: fatigue, hair thinning, cold intolerance, constipation, weight gain, brain fog, low mood. When practitioners rely only on TSH, they may overlook women who are symptomatic despite values within range.
The functional thyroid workup includes TSH, free T4, free T3, reverse T3, anti TPO, and anti thyroglobulin antibodies. Nutritional interventions must address downstream deficiencies and reduce the inflammatory and toxic load on the thyroid.
Functional Lab Markers Worth Knowing
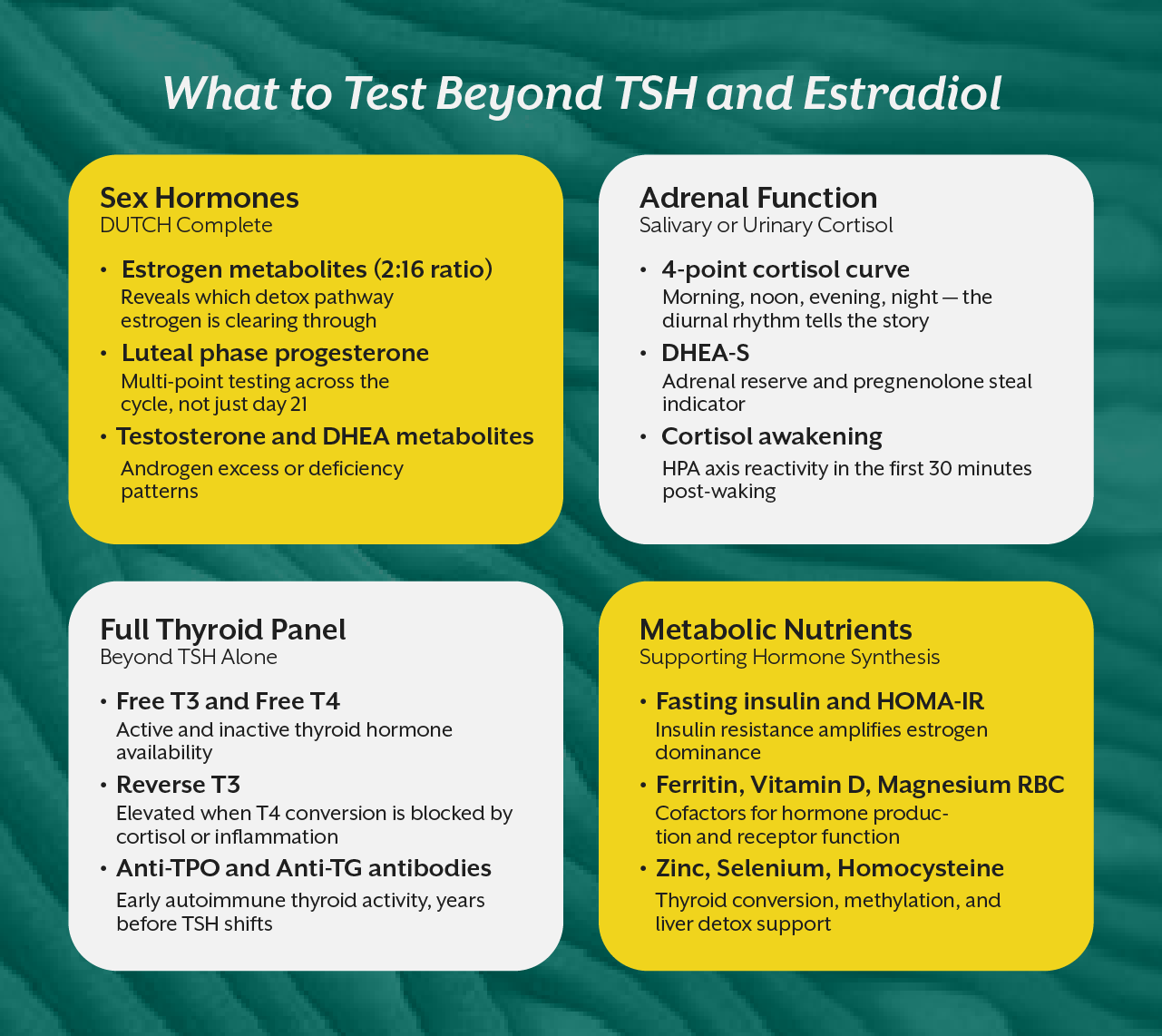
A complete functional hormone assessment for a woman typically includes: DUTCH Complete for sex hormones and their metabolites, a comprehensive thyroid panel, a four point cortisol curve, fasting insulin and HOMA IR for metabolic context, ferritin, vitamin D, magnesium RBC, zinc, selenium, homocysteine, and a full lipid panel. Gut microbiome assessment adds meaningful clinical data when estrogen dominance is present.
This is not the standard of care in most clinics. Learning to order, interpret, and act on these markers is a clinical skill that takes structured education to develop. It can help practitioners move beyond symptom management toward addressing root causes more effectively.
The Nutrition Protocols That Actually Work
Balancing female hormones naturally through nutrition is not about eliminating food groups or following a generic detox. It is precise, targeted, and informed by what the labs reveal.
Across most presentations of hormonal imbalance, a few consistent principles apply. Adequate protein, at least 1.2 to 1.6 grams per kilogram of body weight, supports hormone synthesis and stabilises blood sugar. Blood sugar stability is foundational because insulin dysregulation amplifies estrogen dominance and suppresses progesterone. Colour variety in vegetables ensures phytonutrients that support liver detoxification and estrogen clearance. Seed cycling provides lignans and fatty acids that modulate hormone production across cycle phases. Omega 3 fatty acids reduce the prostaglandin mediated inflammation that drives painful periods. Fermented foods or targeted probiotic support to the estrobolome directly improve estrogen elimination.
These protocols, when mapped to individual lab findings, can support addressing underlying dysfunction alongside symptom management approaches used in conventional care.
Where Practitioners Go Next
Understanding female hormone health at this level is not a small clinical upgrade. It is a complete shift in how you see the body, and it can significantly expand your clinical perspective and approach to patient care.
If this kind of systems thinking resonates with you, iThrive Academy offers two highly relevant programmes worth exploring. The Women's Hormonal Health course is a focused, self-paced certification that goes deep into the endocrine system, menstrual cycle physiology, fertility disorders, perimenopause, and the role of quantum biology in hormonal signalling. At just 5 hours across 11 modules, it is designed for practitioners and health coaches who want clinical-grade knowledge without committing to a full programme.
For those who want the complete clinical foundation, the iThrive Certified Functional Nutrition (iCFN) course is a comprehensive functional nutrition certification designed for clinical application. Over 4 months and 12 comprehensive modules, it covers the entire terrain of chronic disease through a root cause lens, with hormonal health as one of its most richly developed areas.
The women sitting in your clinic or asking you questions deserve practitioners who know more than their TSH number. The knowledge is increasingly accessible to those willing to explore it.




.jpg)