Introduction
The estrobolome is the collection of gut bacteria responsible for metabolising estrogen in the intestinal tract. The liver conjugates estrogen, tagging it for elimination. That conjugated estrogen travels to the gut and is supposed to be excreted through the stool. When the gut microbiome is balanced, this process is fairly efficient.
When gut dysbiosis is present, certain bacterial strains produce excess beta-glucuronidase, an enzyme that strips the conjugation tag from estrogen. Deconjugated estrogen is then reabsorbed through the intestinal wall, re-enters circulation, and adds to the body's total estrogen load. This cycle is called enterohepatic recirculation, and it is a major and underappreciated driver of estrogen dominance in endometriosis.
The connection between endometriosis and gut health goes even further. Research consistently shows that women with endometriosis have measurably different gut microbiome profiles compared to women without the condition. There is more dysbiosis, higher intestinal permeability, and greater systemic inflammation. These are not side effects of endometriosis. They are part of the mechanism sustaining it.
For practitioners, this means the gut is not a bystander in endometriosis management. It is an active participant. And for women trying to understand why their symptoms persist despite medical treatment, the state of their gut microbiome is a genuinely meaningful clinical variable.
Because endometriosis rarely exists in isolation, many women also experience wider patterns of hormonal dysfunction involving estrogen, progesterone, cortisol, insulin, and thyroid hormones, explored in detail in our blog, ‘Women’s Hormonal Imbalance: A Functional Nutrition Guide.
The Anti-Inflammatory Endometriosis Diet: What the Evidence Actually Supports

Let us get into what this means practically, because this is often where the conversation either becomes vague or unhelpfully restrictive.
Endometriosis is an inflammatory condition. Prostaglandins, particularly the pro-inflammatory prostaglandin E2, are elevated in endometriotic tissue and drive much of the pain and progression. Nutrition directly influences prostaglandin synthesis through its effect on fatty acid metabolism. This is why the endometriosis diet is not arbitrary, rather it is pharmacologically relevant.
The most consistently supported dietary direction in endometriosis functional nutrition research points toward a few clear principles. Omega-3 fatty acids from sources like fatty fish, flaxseeds, and walnuts reduce pro-inflammatory prostaglandin synthesis. A diet rich in fibre from diverse plant sources supports gut microbiome diversity and facilitates estrogen excretion through the bowel. Cruciferous vegetables supply indole-3-carbinol and DIM, which shift estrogen metabolism toward less proliferative pathways. Polyphenol-rich foods like berries, and turmeric directly modulate NF-kB, the master switch of inflammatory gene expression.
For women managing endometriosis naturally in India, this translates well into traditional food patterns. A diet built around dal, sabzi, fish, chicken, free-range eggs and minimal refined carbohydrate is closer to therapeutic than most women realise. The key adjustments tend to be more about what to reduce than what to add. Where Indian diets typically fall short in the endometriosis context is in refined carbohydrate load from white rice and maida-based foods, both of which drive the insulin-aromatase signalling that feeds local estrogen production in lesion tissue.
Foods to Avoid with Endometriosis: The Inflammatory Drivers

This is perhaps the most searched question women with endometriosis ask, and the answer is genuinely useful when it is clinically grounded rather than generic.
Processed meat
It increases arachidonic acid availability in the body, which shifts prostaglandin synthesis toward the pro-inflammatory pathway. Several observational studies have associated higher red meat intake with increased endometriosis risk and symptom severity.
Refined sugar and high glycaemic foods
It drives insulin spikes, which increase aromatase activity and therefore local estrogen production within endometriotic tissue. Blood sugar instability is not metabolically neutral in endometriosis, it actively feeds the hormonal environment that promotes lesion growth.
Alcohol
It impairs liver phase one and phase two detoxification, directly reducing the liver's capacity to conjugate estrogen for elimination. Even moderate alcohol consumption has been associated with elevated circulating estrogen levels.
Conventional dairy and non-organic animal products
These are more nuanced conversations. The concern is not dairy categorically but the presence of exogenous hormones and saturated fat in conventionally raised animal products, both of which can influence estrogen load and inflammatory signalling.
Trans fats and highly processed vegetable oils
It suppresses the omega-3 to omega-6 ratio that governs prostaglandin balance, tipping the body toward a chronic inflammatory state.
The Supplement Protocol Worth Knowing
Endometriosis natural treatment through supplementation works best when targeted rather than generic. These are the nutrients with the strongest evidence base.
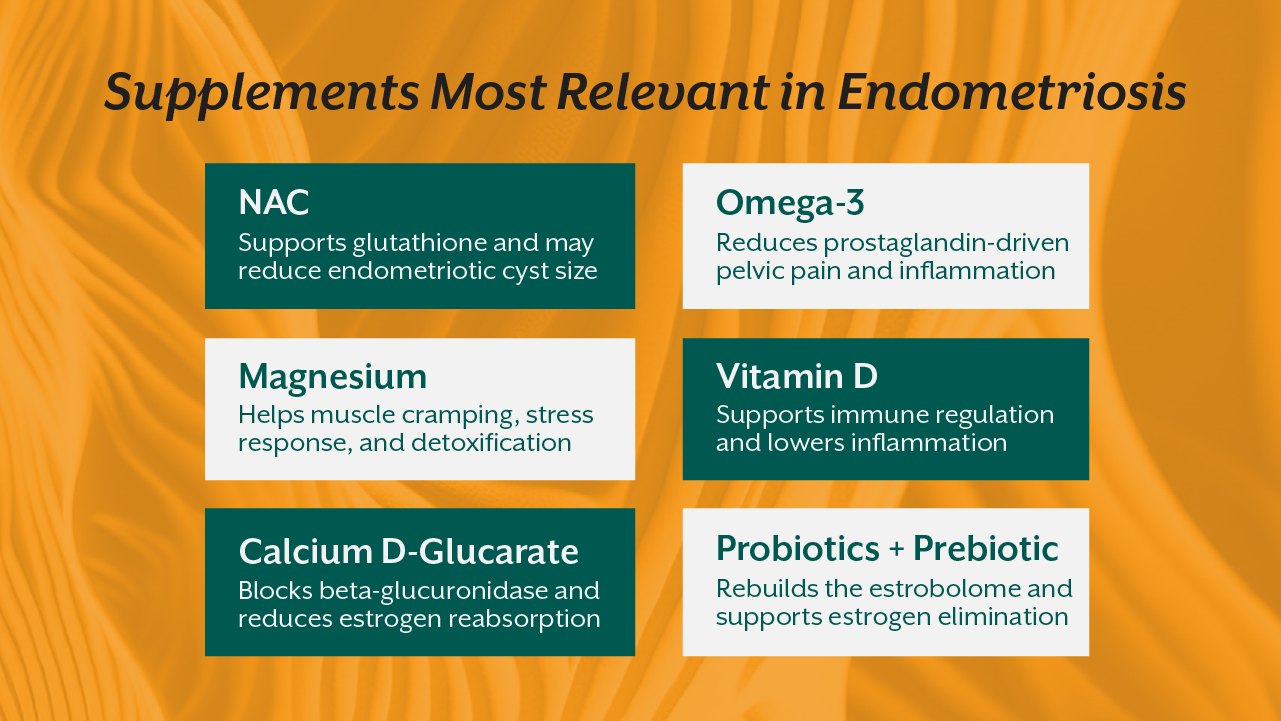
N-acetyl cysteine (NAC)
NAC has shown remarkable results in clinical studies. A randomised trial in Italy found that NAC supplementation reduced endometriotic cyst size in a clinically meaningful proportion of participants, with a significant number avoiding planned surgery. The mechanism involves glutathione support and reduction of oxidative stress within lesions.
Marine Omega-3
Omega 3 at therapeutic doses reduce prostaglandin E2 synthesis and have been shown to reduce pelvic pain severity in women with endometriosis.
Magnesium
Magnesium addresses the uterine muscle cramping component and supports liver detoxification enzymes. Deficiency is extremely common in women with endometriosis.
Vitamin D
Vitamin D3 K2 has direct anti-inflammatory effects and influences immune modulation. Women with endometriosis consistently show lower vitamin D levels than controls in research populations, and correction of deficiency has been associated with reduced symptom burden.
Calcium D-glucarate
It directly inhibits beta-glucuronidase activity in the gut, blocking estrogen reabsorption at the intestinal level. This is one of the most targeted supplements available for the estrobolome piece of endometriosis management.
Probiotics and prebiotic fibre
It supports microbiome diversity and helps rebuild the gut environment that enables healthy estrogen clearance.
What This Means Clinically: The Gap in Standard Care
The reason endometriosis diet India remains such an underserved search and clinical conversation is that it requires thinking across systems simultaneously. The gynaecologist thinks about the uterus and ovaries. The gastroenterologist thinks about the gut. Nobody is standing in the middle looking at how these systems speak to each other.
That integrative middle ground is exactly where functional nutrition operates, where the most meaningful clinical improvement happens, not through a single intervention but through understanding the estrogen dominance, gut dysbiosis, systemic inflammation loop and addressing all three deliberately.
This is not about replacing surgical or medical management where it is genuinely needed. It is about recognising that for a condition as complex and chronic as endometriosis, nutrition and gut health are not optional add-ons. They are part of the mechanism.
Where to Build This Knowledge
If working at this level of clinical depth with female patients interests you, this is exactly the territory covered in iThrive Academy's Women's Hormonal Health course. It is a focused, self-paced certification exploring the endocrine system, estrogen metabolism, cycle physiology, and fertility disorders with the kind of mechanistic rigour that makes you actually useful to women in your clinic or to yourself.
For practitioners who want the full systems framework, the iThrive Certified Functional Nutrition programme trains you to see the gut, hormones, inflammation, and nutrition as one integrated clinical picture across 12 modules over four months. It is the foundation from which managing conditions like endometriosis becomes something genuinely solvable rather than endlessly managed.
The gap in care for women with endometriosis is large, and it exists precisely because no single specialty owns the full picture. Practitioners who understand the gut-hormone connection and who can read a GI Map alongside a DUTCH test and design a protocol that addresses both are genuinely rare. Building that knowledge is exactly what iThrive Academy trains people to do, drawn from a live clinical practice that has worked with over a thousand practitioners and patients across India and beyond.
References
https://pmc.ncbi.nlm.nih.gov/articles/PMC8508982/




.jpg)