Introduction
If you are a practitioner, educator, or advanced learner, you already know something important. Hypertension is rarely just a number. It is a pattern.
Yet most treatment models still revolve around one question. How do we lower blood pressure?
That question is necessary. It is not sufficient.
A real care plan for hypertension must answer deeper questions. Why is regulation failing? Which control system is dominant in this patient? Is the elevation neural, vascular, renal, metabolic, or inflammatory in origin? And most importantly, what needs to change so that the system becomes adaptive again rather than simply suppressed?
In clinical practice, many practitioners feel stuck between two worlds. Conventional guidelines focus on medication algorithms. Lifestyle advice is often generic and poorly implemented. Functional medicine speaks of root causes but sometimes lacks structured sequencing.
What if we integrate both?
This blog is not about replacing medication. It is about designing a layered, clinically intelligent care plan for hypertension that addresses acute control, system drivers, and long term prevention of hypertension through regulatory restoration.
You are not here to memorise tips. You are here to refine your clinical reasoning.
Let us build this step by step.
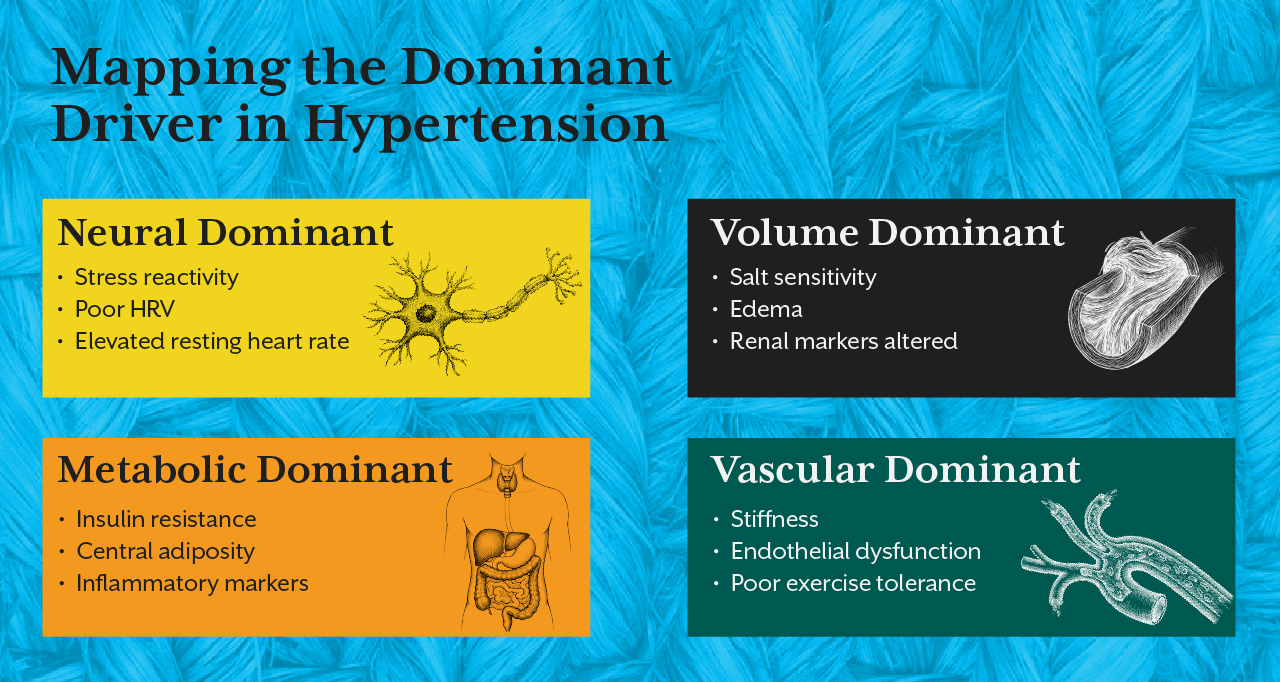
Step One: Define the Dominant Regulatory Driver
Before designing any treatment of hypertension, you must identify which system is most dysregulated.
Blood pressure is governed by neural tone, vascular resistance, fluid volume, endocrine signalling, and metabolic energy availability. A care plan that does not clarify the dominant driver will always remain reactive.
For example, a patient with high sympathetic drive, poor heart rate variability, shallow breathing, and stress reactivity requires a very different strategy compared to someone with salt sensitivity, edema, and renal driven pressure elevation.
This is where many practitioners struggle. They treat the number. They do not map the pattern.
The iThrive Academy blog Decoding Functional Sports Nutrition: How Electrolytes and HRV Define True Athletic Recovery explains beautifully how autonomic balance determines performance capacity. The same principle applies here. If sympathetic dominance persists, vascular tone remains elevated. Pressure rises not because vessels are damaged but because neural output is excessive.
A proper care plan for hypertension begins with pattern recognition. Without this, even the best protocols fail.
Step Two: Stabilise Without Ignoring Physiology
There are times when medication is necessary. Severe hypertension increases cardiovascular risk and must be stabilised. Ignoring pharmacology in the name of functional medicine is irresponsible.
However, medication should be understood as a regulatory stabiliser, not a cure.
A thoughtful care plan for hypertension integrates medication when needed while simultaneously investigating the underlying drivers. For example, beta blockers reduce sympathetic responsiveness. But if chronic stress patterns and poor sleep architecture persist, neural dominance remains.
ACE inhibitors may reduce hormonal amplification through RAAS modulation. Yet if insulin resistance is driving sodium retention and endothelial dysfunction, metabolic correction must accompany drug therapy.
This layered thinking differentiates protocol based practice from physiology based care.
In the iThrive Academy blog Insulin Resistance The Silent Phase Before Type 2 Diabetes, we see how metabolic dysregulation precedes overt disease. The same applies here. Insulin resistance increases sodium retention, sympathetic activation, and vascular stiffness long before blood pressure readings become alarming.
A functional care plan addresses metabolic drivers even when glucose levels appear normal.
Step Three: Address Neural Regulation Directly
Many hypertension care plans mention stress reduction casually. Very few quantify it.
Neural regulation is not a motivational topic. It is physiology.
Chronic sympathetic activation increases vascular tone, elevates cardiac output, and enhances renal sodium retention. If autonomic imbalance persists, even dietary sodium restriction may produce limited results.
A clinical and functional medicine approach includes structured autonomic interventions. These may involve breathing retraining, sleep restoration, circadian rhythm alignment, and progressive stress adaptation protocols.
When heart rate variability improves, vascular reactivity often improves. When sleep architecture stabilises, nocturnal dipping patterns normalise.
The prevention of hypertension in high risk individuals often begins here. Before numbers rise dramatically, autonomic dysregulation is usually detectable.
Practitioners trained at iThrive Academy learn to assess autonomic patterns, metabolic markers, and endocrine interplay together. This system's lens changes how care plans are constructed.




.jpg)