Introduction
If you have studied nutrition formally, you have likely been taught to view Polycystic Ovary Syndrome through a familiar lens. Reduce calories. Encourage weight loss. Improve insulin resistance. Restore cycles.
It sounds logical. It sounds structured. It sounds measurable.
And yet, in clinical practice, you already know what happens next.
The patient follows a calorie restricted plan. She lost a few kilograms. The cycle is not regulated. The acne persists. The cravings return. The weight plateaus. The stress worsens.
The problem is not effort. The problem is not discipline. The problem is that most nutrition courses reduce PCOS to an energy balance equation when it is fundamentally a cellular energy disorder.
PCOS is not a failure of willpower. It is a failure of signaling.
At iThrive Academy, we teach practitioners to shift their thinking from calorie mathematics to mitochondrial physiology. Because unless you understand how a cell senses energy, no macronutrient prescription will hold long term.
Let us unpack what most courses get wrong and what a metabolism first framework actually looks like.
PCOS Is Not Just Ovarian, It Is Bioenergetic
Most syllabi begin with the ovaries. Follicles. LH and FSH ratios. Testosterone. Ultrasound morphology.
But the ovary does not operate in isolation. It is one of the most energy sensitive organs in the female body. Ovulation is metabolically expensive. Follicular maturation requires ATP, redox balance, and mitochondrial density.
When mitochondria are dysfunctional, ovarian tissue cannot interpret hormonal signals correctly. Insulin receptors become blunted. Androgen synthesis increases. Follicles stall.
This is why in our previously published blog, Decoding Functional Sports Nutrition: How Electrolytes and HRV Define True Athletic Recovery, we emphasized that recovery physiology depends on cellular energy efficiency and nervous system balance. The same regulatory logic applies here. Different systems. Same principle.
If a muscle cannot recover without mitochondrial competence, why would an ovary ovulate without it?
Insulin Resistance Is a Signaling Disorder, Not a Sugar Problem
Many courses teach insulin resistance as excessive carbohydrate intake. That framing is incomplete.
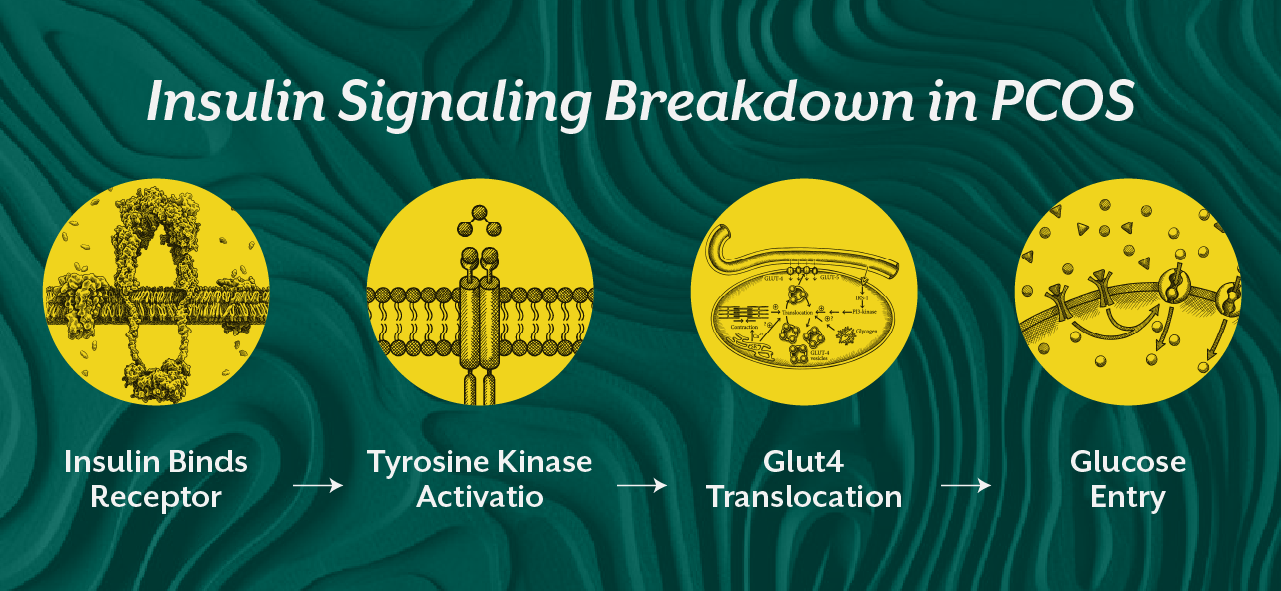
Insulin resistance in PCOS is a signaling amplification error. The pancreas produces more insulin not because glucose is always high, but because peripheral tissues are not responding efficiently. At the cellular membrane, insulin binds to its receptor. This activates a cascade involving tyrosine kinase activity and GLUT4 translocation. In a metabolically flexible system, glucose enters the cell and is oxidized. In a dysfunctional system, oxidative stress and lipid intermediates impair this signaling cascade. The receptor is present. The hormone is present. The response is weak.
The result is compensatory hyperinsulinemia. And insulin in the ovary behaves as a co-gonadotropin. It stimulates theca cells to produce more androgens. The patient does not have a willpower problem. She has a receptor sensitivity problem. This is where many practitioners feel stuck. They prescribe low glycemic diets, but they do not address mitochondrial density, inflammatory tone, or skeletal muscle inactivity.
In our blog, Insulin Resistance Is a Whole Body Disorder, we explained how muscle, liver, adipose tissue, and pancreas form an integrated metabolic network. PCOS is that same network dysfunction expressed through reproductive tissue.
The Nervous System Is the Missing Chapter in Most Courses
You cannot teach PCOS properly without teaching the nervous system.
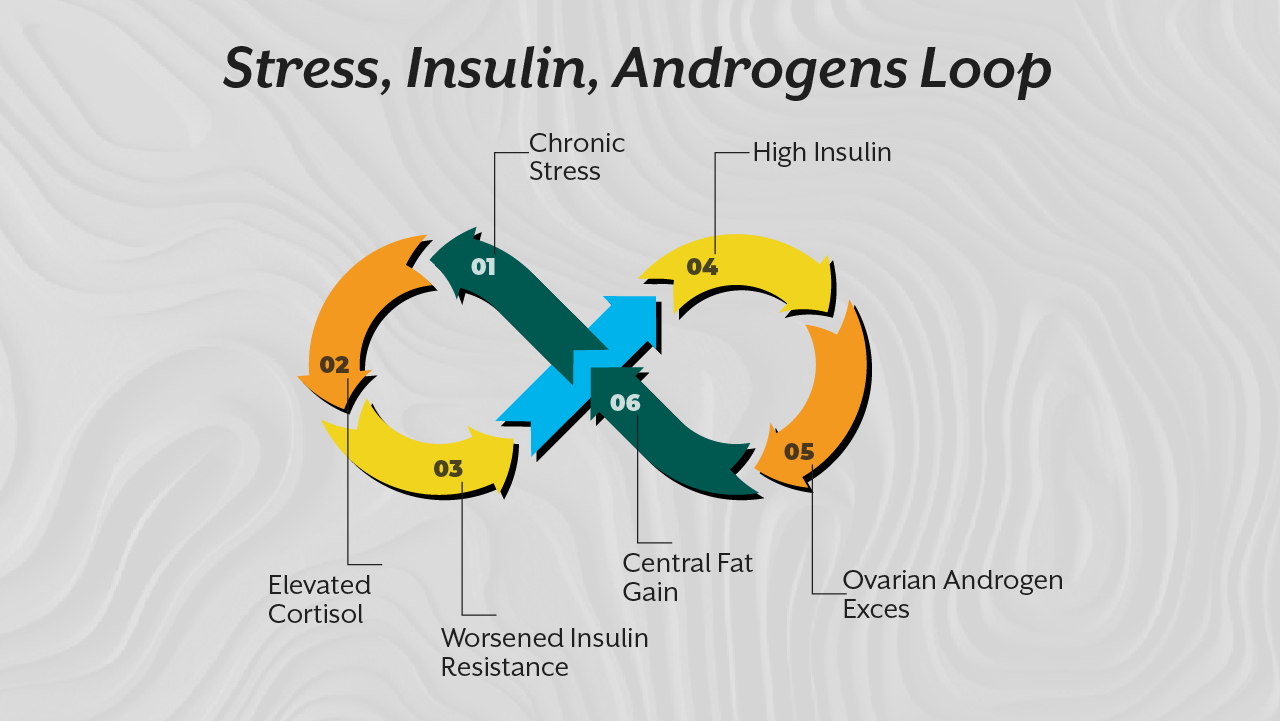
Chronic sympathetic activation elevates cortisol. Elevated cortisol worsens insulin resistance. Insulin resistance increases androgen production. Androgen excess worsens central adiposity. Central adiposity drives inflammatory cytokines.
It is a loop.
Most nutrition programs ignore this because stress is difficult to quantify. But practitioners know the pattern. The patient with PCOS often reports anxiety, sleep disruption, irregular appetite signals, and fatigue.
The HPA axis and HPO axis are not separate. They communicate continuously.
Mitochondria are also stress sensors. When stress is chronic, reactive oxygen species increase. Oxidative stress damages mitochondrial DNA. ATP production declines. The ovary becomes less responsive to FSH signaling.
You cannot calories restrict your way out of sympathetic dominance.
You need parasympathetic restoration. You need muscle contraction. You need circadian alignment.
This is what we emphasize inside the iCFN curriculum at iThrive Academy. Practitioners must understand regulatory physiology, not just food charts.
Why Calorie Restriction Often Backfires
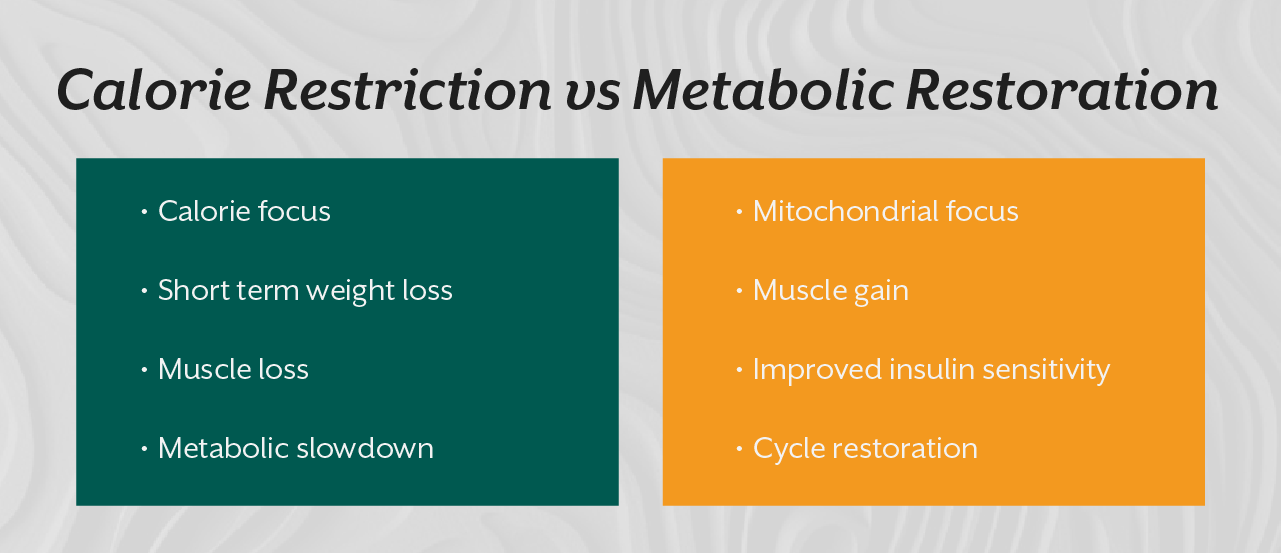
Calorie restriction without metabolic repair can reduce resting metabolic rate.
When energy intake drops significantly, thyroid signaling may reduce. Leptin decreases. The body interprets the deficit as a threat. In women with PCOS who already have impaired metabolic flexibility, this can intensify fatigue and stress.
If skeletal muscle mass is low and mitochondrial density is poor, a calorie deficit simply reduces intake without increasing oxidation. The patient feels deprived but metabolically stagnant.
This is why resistance training is not optional. Skeletal muscle is the largest glucose disposal organ in the body. It increases GLUT4 independent of insulin. It enhances mitochondrial biogenesis. It improves insulin sensitivity at the tissue level.
When practitioners focus only on calories, they ignore tissue quality.
A 5 kilogram weight loss achieved through muscle building and visceral fat reduction is metabolically different from a 5 kilogram loss achieved through severe restriction and lean mass loss.
Cellular metabolism determines outcome quality.
Reframing PCOS as a Metabolic Education Problem
When you view PCOS through a cellular metabolism lens, your interventions change.
You prioritize protein adequacy not for weight loss but for SHBG synthesis and muscle repair.
You prioritize omega-3 fats not for calories but for membrane fluidity and receptor function.
You address circadian rhythm because melatonin is a mitochondrial antioxidant.
You teach breath work and stress modulation because parasympathetic dominance improves insulin sensitivity.
You stop asking, how many calories did she eat?
You start asking, how efficiently are her cells generating energy?
This shift changes your authority as a practitioner.
Patients sense when you understand mechanisms. They sense when you are treating the root rather than suppressing symptoms.
Inside the iCFN program at iThrive Academy, we train learners to interpret labs beyond reference ranges, to connect insulin to androgen synthesis, to link stress physiology to ovarian function, and to design interventions that restore signaling rather than impose restriction.
Because the future of metabolic health education cannot remain stuck in calorie arithmetic.
Key Takeaway
Most nutrition courses fail in PCOS education because they teach energy balance without teaching energy biology. PCOS is not fundamentally a calorie disorder. It is a disorder of mitochondrial efficiency, insulin signaling, nervous system regulation, and tissue responsiveness. When practitioners shift from restriction to restoration, from weight loss to metabolic flexibility, outcomes change. Cycles regulate. Inflammation declines. Insulin normalizes. And the patient regains physiological resilience. If you want to practice at a higher level, you must think at the level of the cell.




.jpg)