Introduction
If you are a practitioner, educator, or advanced learner, you have likely encountered this clinical paradox repeatedly:
- The patient reports clear thyroid symptoms such as fatigue, hair loss, cold intolerance, weight gain, and mood changes yet laboratory reports indicate normal thyroid levels.
- TSH is within range.
- T4 is technically adequate.
- Treatment is not indicated.
- Case closed.
But clinically, the case is far from closed.
Patients continue to experience thyroid disease symptoms despite “normal” results. Some are told their symptoms are psychological. Others are reassured repeatedly while physiological dysfunction progresses quietly. Many begin thyroid treatment only after years of metabolic deterioration.
This is not simply a diagnostic challenge. It is an educational limitation.
Most thyroid education teaches biochemical thresholds but not physiological interpretation. It teaches hormone measurement but not hormone signaling. It teaches treatment algorithms but not adaptive compensation.
And that is precisely where clinical reasoning begins to fail.
At iThrive Academy, one of the most common realizations learners report is this: they were trained to read thyroid numbers, but not to understand thyroid physiology.
This article explores what conventional thyroid education overlooks and the clinical framework required to interpret thyroid function meaningfully.
Thyroid Physiology Is Taught as Hormone Production, Not Hormone Signaling
Most training begins with structure.
- The thyroid gland produces T4.
- T4 converts to T3.
- TSH regulates production.
While accurate, this model is incomplete.
Because thyroid hormone function is not determined solely by production, it is determined by signaling effectiveness at the cellular level.
A patient can produce sufficient hormone but still experience functional hypothyroidism if:
- Conversion to active T3 is impaired
- Cellular receptor sensitivity is reduced
- Inflammatory signaling blocks hormone action
- Nutrient cofactors for metabolism are deficient
- Stress hormones alter tissue responsiveness
Conventional teaching rarely emphasizes this distinction.
As a result, clinicians learn to evaluate supply but not utilization.
This explains why thyroid test normal but symptoms is one of the most common clinical scenarios and one of the least understood educationally.
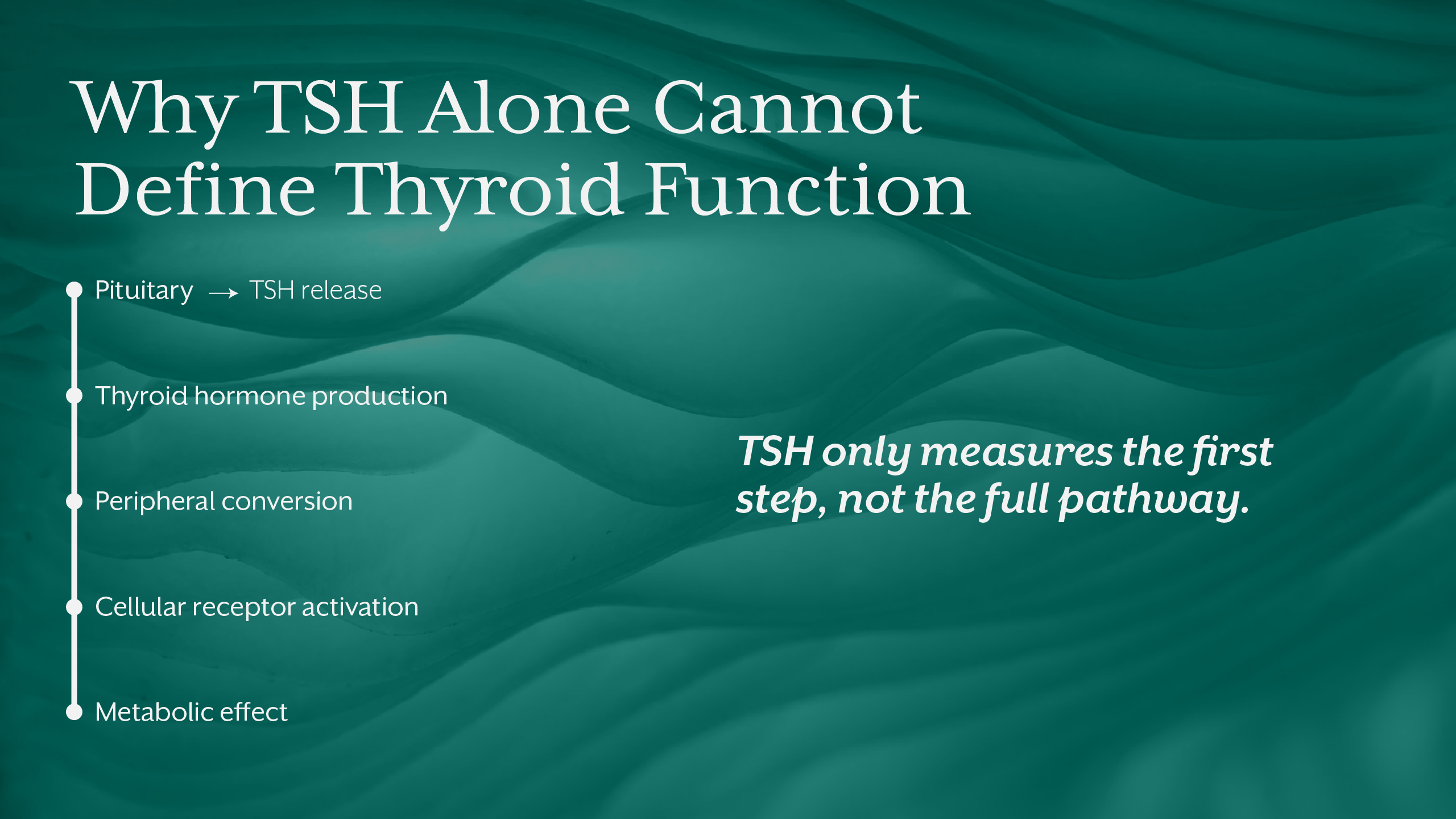
The Overreliance on TSH as a Diagnostic Anchor
Thyroid education places disproportionate emphasis on TSH.
It is treated as the primary indicator of thyroid status.
In reality, TSH reflects pituitary response, not tissue-level thyroid activity.
TSH can remain within range while:
- Peripheral conversion is impaired
- Reverse T3 is elevated
- Cellular energy production is reduced
- Inflammatory cytokines interfere with receptor binding
This is why patients with normal TSH but thyroid symptoms represent a predictable physiological pattern, not an anomaly.
TSH is a regulatory signal, not a direct measurement of metabolic effect.
When thyroid misdiagnosis occurs, it is often because regulatory signals are mistaken for functional outcomes.
Autoimmunity Is Often Detected Late Because Antibody Testing Is Underutilized
Many practitioners are trained to diagnose Hashimoto’s thyroiditis only after overt dysfunction appears.
However, thyroid antibodies often rise years before hormone disruption.
During this period, patients may present with fluctuating symptoms, inflammatory patterns, and metabolic instability yet remain within biochemical reference ranges.
Without antibody testing, early thyroiditis is easily missed.
This creates a diagnostic delay that allows progressive immune-mediated tissue damage.
Autoimmune thyroid disease is therefore frequently treated as an endocrine disorder when it is fundamentally an immune regulation disorder.
This conceptual notion is explored extensively in the iThrive Academy blog: “Insulin Resistance as a Pre-Diagnostic State: Why Type 2 Diabetes Is a Late Label.”
The same infrastructure logic applies to thyroid autoimmunity, because dysfunction precedes diagnosis.
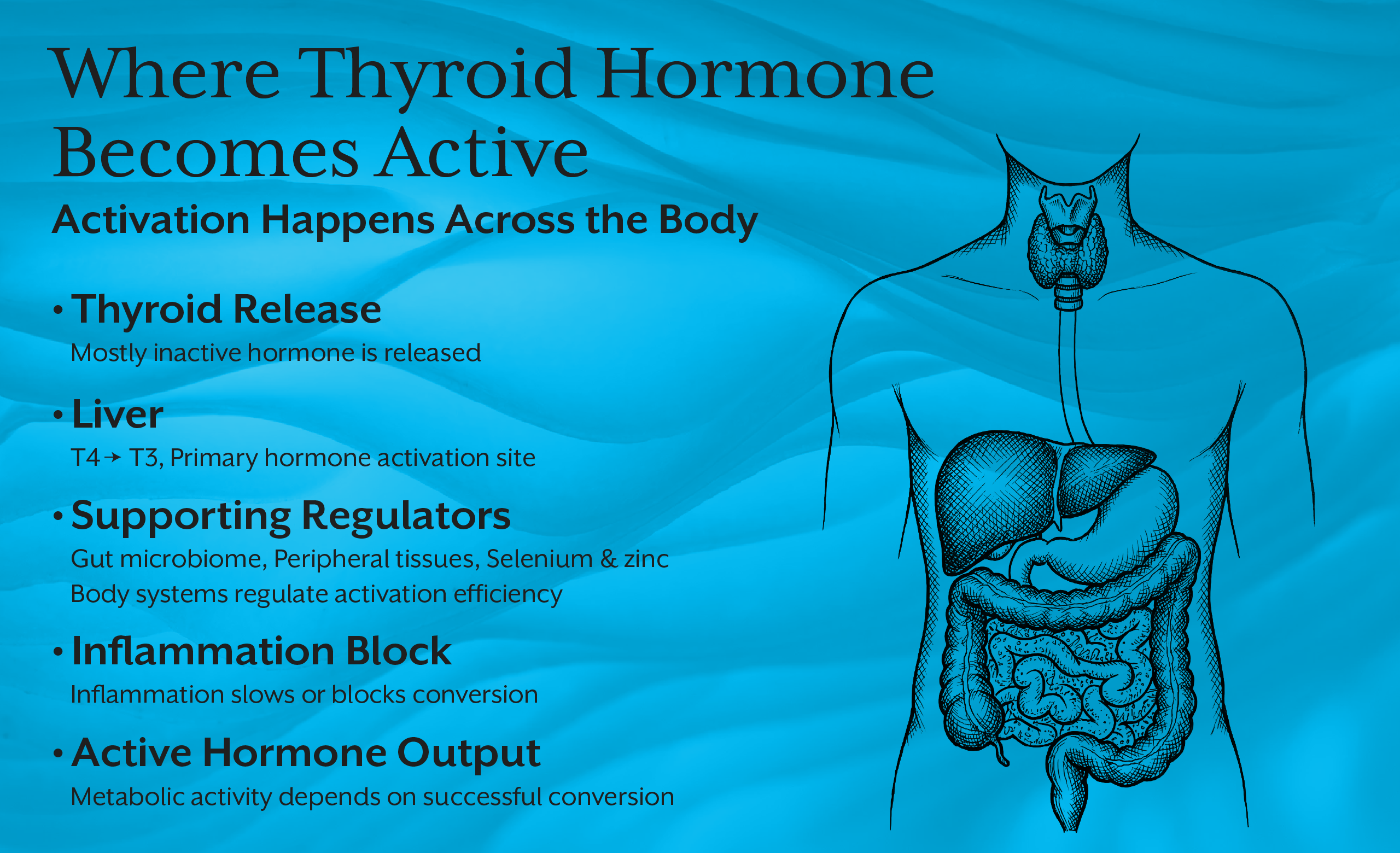
The Missing Role of Conversion Physiology
One of the most underemphasized areas in thyroid education is hormone conversion.
T4 is a storage hormone.
T3 is the active metabolic signal.
Conversion occurs primarily in the liver, gut, and peripheral tissues, not the thyroid gland itself.
This means thyroid function depends heavily on systemic metabolic health.
Factors affecting conversion include:
- Liver detoxification capacity
- Gut microbiome integrity
- Selenium status
- Chronic inflammation
- Cortisol patterns
- Nutrient sufficiency
When conversion is impaired, patients develop subclinical hypothyroidism symptoms despite adequate production. This is not gland failure. It is systemic metabolic dysregulation.
Thyroid Function Cannot Be Interpreted Without Metabolic Context
Thyroid hormones regulate energy expenditure.
But energy availability regulates thyroid signaling in return.
Caloric restriction, chronic stress, inflammation, infection, and nutrient deficiency all influence thyroid adaptation.
In many cases, reduced thyroid activity represents metabolic conservation, and not pathology.
This adaptive physiology is rarely taught.
Instead, thyroid function is framed as either normal or abnormal, without acknowledging that the body actively recalibrates metabolism to maintain survival.
When adaptation is misinterpreted as failure, treatment may suppress protective mechanisms rather than address underlying drivers.
Why Thyroid Treatment Fails in Many Patients
When thyroid treatment focuses solely on hormone replacement, but underlying physiology remains unchanged, symptom resolution is inconsistent.
Treatment may fail because:
- Inflammation continues to block receptor activity
- Nutrient deficiencies impair cellular metabolism
- Gut dysfunction alters absorption
- Stress hormones override metabolic signaling
- Immune activity persists
In such cases, medication adjusts circulating hormone but not functional responsiveness. This is why many patients remain symptomatic even after treatment initiation. Clinical success requires system-level restoration, not biochemical correction alone. This systems-based reasoning is foundational within the iThrive Academy blog: “What Makes a Thyroid Supplement Effective? The Science of Bioavailability and Nutrient Activation” The same principle applies to medication, bioavailability and cellular activation matter as much as dosage.
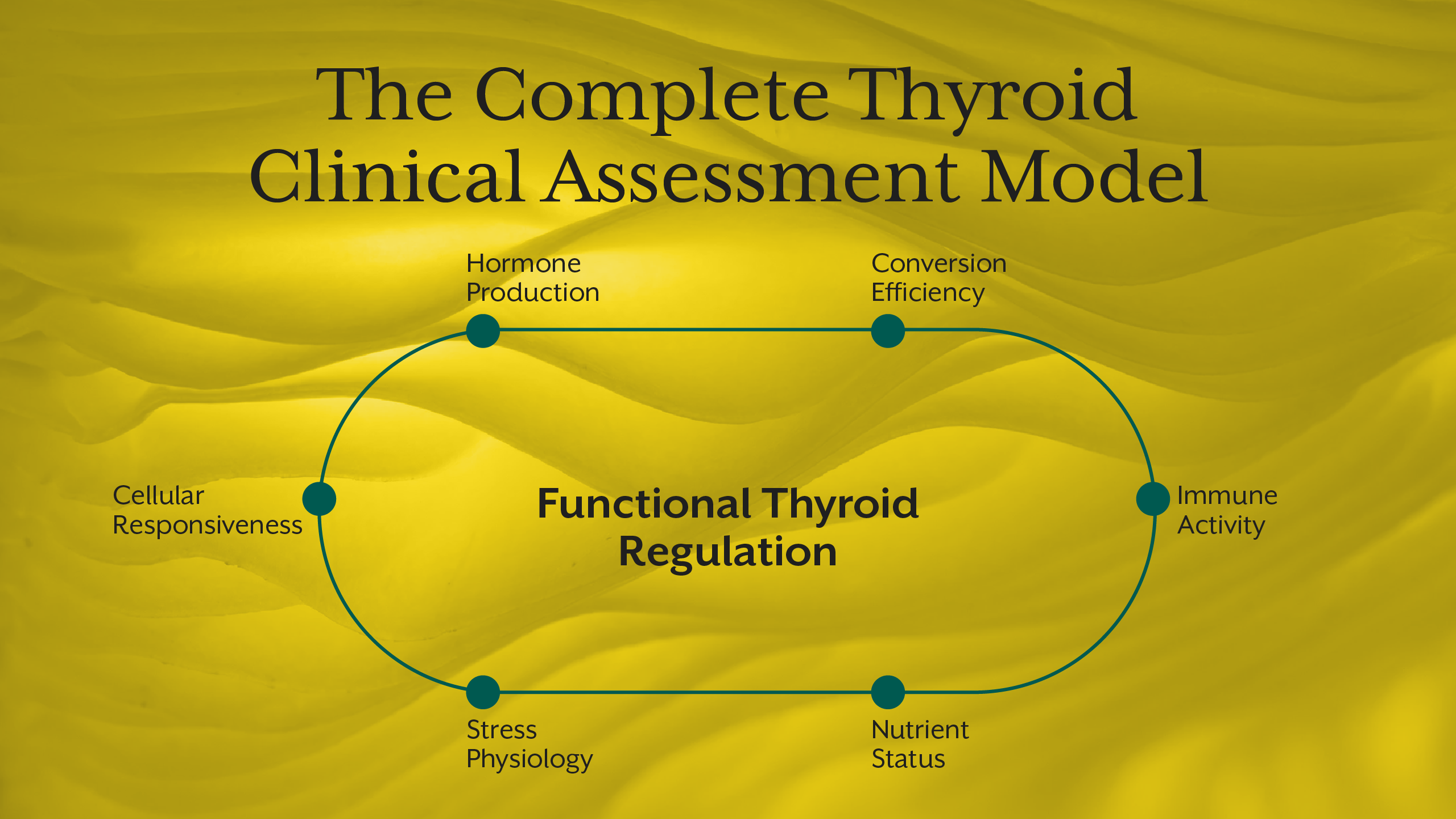
The Clinical Framework Missing from Most Thyroid Education
If thyroid physiology is systemic, thyroid assessment must be systemic.
A meaningful clinical framework integrates:
- Hormone production
- Hormone conversion
- Immune activity
- Nutrient availability
- Stress physiology
- Mitochondrial function
- Tissue responsiveness
When learners are trained to evaluate these domains collectively, thyroid patterns become interpretable rather than confusing.
This integrative clinical reasoning is central to structured training such as the iThrive Certified Functional Nutrition program and the specialized Thyroid Educator short course, where learners are trained to interpret thyroid physiology across systems rather than in isolation.
What Practitioners Must Unlearn
Clinical education often requires conceptual correction.
Practitioners must unlearn that:
- Thyroid function equals gland output.
- Normal labs equal normal physiology.
- Autoimmunity begins at diagnosis.
- Hormone replacement restores function fully.
These assumptions simplify teaching but distort clinical reality.
True thyroid assessment requires pattern recognition across immune, metabolic, neurological, and endocrine systems simultaneously.
This is the framework that conventional training rarely provides but clinical practice demands.
Key Takeaway
Thyroid dysfunction is rarely a single-gland disorder. It is an emergent pattern arising from immune regulation, metabolic signaling, nutrient status, stress physiology, and cellular responsiveness. Conventional thyroid education often isolates hormone production while overlooking the broader regulatory network that determines hormone effectiveness. This reductionist model explains why thyroid symptoms persist despite normal labs, why treatment outcomes vary widely, and why autoimmune thyroid disease is frequently detected late. A clinically meaningful thyroid framework must interpret signaling, adaptation, and system integration, not simply hormone concentration. When practitioners learn to assess thyroid function within metabolic context, diagnostic clarity improves and intervention becomes physiologically aligned rather than algorithmically driven.




.jpg)