Introduction
If you were trained in traditional nutrition, chances are obesity was introduced to you early as a calorie imbalance problem. Eat less. Move more. Reduce portions. Increase activity. If weight doesn’t drop, compliance must be the issue.
But then real life intervenes.
You meet clients who eat “clean,” track calories meticulously, exercise consistently, and yet struggle with weight gain, metabolic slowdown, fatigue, and hormonal disruption. You start noticing that the education you received doesn’t explain what you’re seeing in practice.
This is not because obesity is mysterious.
It is because obesity is taught out of sequence.
Traditional nutrition education tends to focus on outcomes rather than processes, numbers rather than biology, and interventions rather than adaptations. In doing so, it unintentionally trains practitioners to treat obesity as a behavioral failure instead of a complex, adaptive metabolic response.
This blog is written for learners, educators, and practitioners who have sensed that disconnect and want to understand where obesity education goes wrong, and how science actually explains obesity development.
Obesity Is Taught Backwards - Starting at the End of the Story
In most nutrition curricula, obesity is introduced at the diagnostic endpoint. Students learn to identify obesity through BMI cut-offs, waist circumference, body fat percentage, and weight categories. Interventions follow immediately: hypocaloric diets, exercise prescriptions, and behavior modification.
What’s missing is the timeline.
Obesity does not begin with excess fat mass. It begins years earlier with subtle shifts in metabolic regulation: rising insulin levels, altered energy sensing, stress-driven adaptations, sleep disruption, inflammatory signaling, and hormonal compensation. These processes precede visible weight gain and remain largely invisible in conventional education.
When obesity is taught from the endpoint backward, learners never fully understand why the body resists weight loss or why calorie restriction often worsens metabolic outcomes long-term. The education model unintentionally frames obesity as a static state rather than a progressive biological adaptation.
Compensation - The Phase Obesity Education Rarely Teaches
One of the most critical omissions in obesity education is the concept of metabolic compensation.
Before dysfunction, the body adapts. Insulin secretion increases to maintain glucose control. Adipose tissue expands to safely store excess energy. Stress hormones mobilize fuel. Appetite signaling adjusts to perceived energy needs. From a survival standpoint, these changes are protective.
From an educational standpoint, they create blind spots.
Because glucose levels may remain normal and overt disease markers are absent, learners are taught that “nothing is wrong yet.” This reinforces the false idea that obesity appears suddenly rather than emerging gradually through years of compensation.
This same blind spot is explored deeply in the iThrive Academy blog “Insulin Resistance as a Pre-Diagnostic State: Why Type 2 Diabetes Is a Late Label”, which highlights how metabolic dysfunction can exist long before clinical thresholds are crossed. The same logic applies to obesity: by the time weight gain is obvious, metabolic strain has already been present for years.
Obesity Is Taught as a Tissue Problem, Not a Communication Problem
Another educational limitation is the way obesity is compartmentalized.
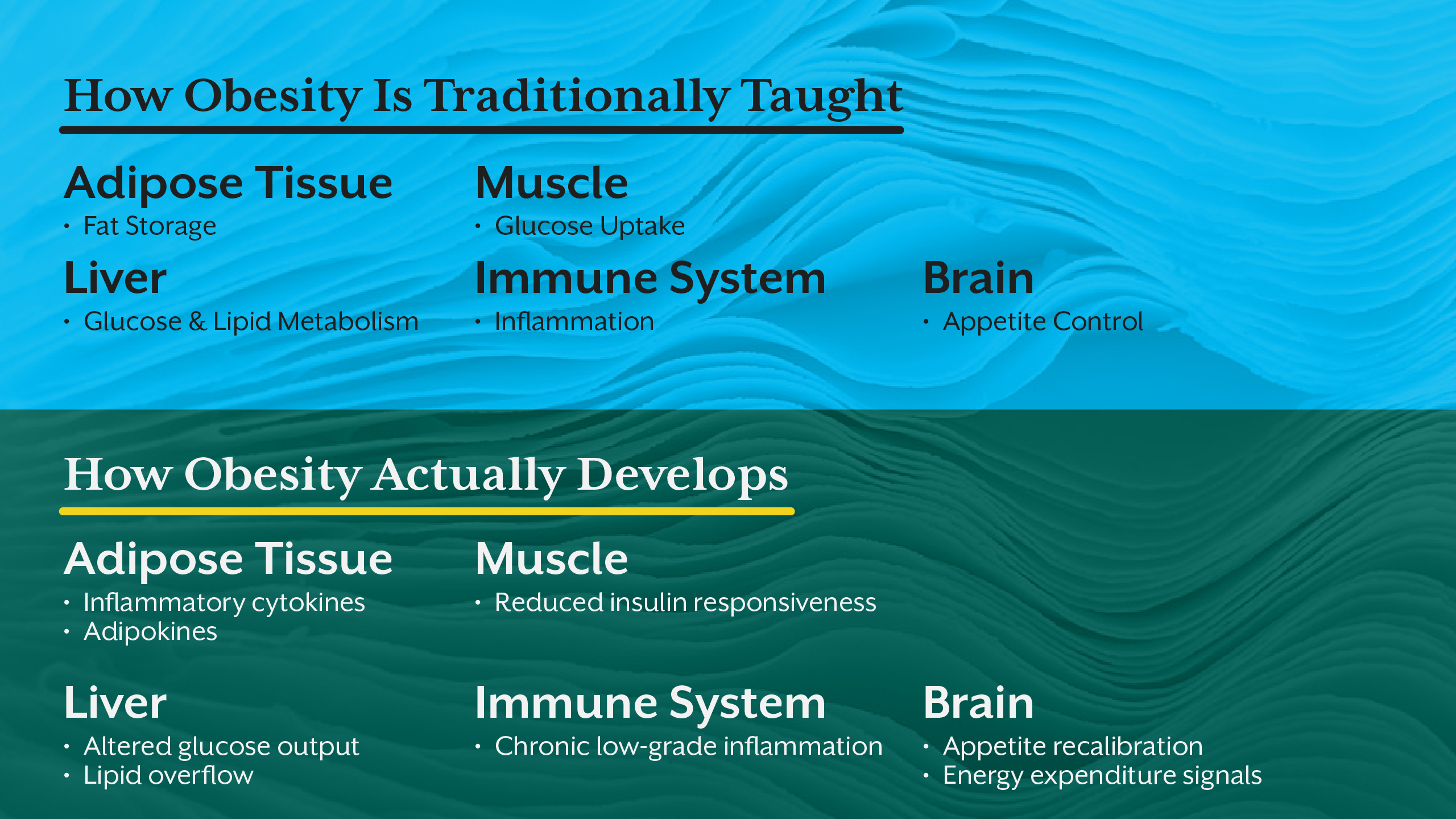
Students learn about adipose tissue in one chapter, insulin in another, hormones elsewhere, and inflammation as a separate topic. Rarely are these systems taught as interconnected signaling networks.
Obesity, however, does not arise from one tissue failing. It emerges when communication between tissues breaks down. Adipose tissue sends inflammatory and endocrine signals. The liver alters glucose and lipid handling. The brain recalibrates appetite and energy expenditure. The immune system amplifies low-grade inflammation. Muscle becomes less responsive to insulin.
When education isolates these systems, learners struggle to see obesity as a network-level disorder, not a single-organ problem. This fragmentation limits clinical reasoning and reinforces reductionist interventions.
Food Is Over-Taught, Biology Is Under-Taught
Traditional nutrition education excels at teaching food groups, dietary guidelines, calorie math, and macronutrient distribution. What it often underemphasizes is how cells sense energy and decide whether to store or burn fuel.
Key biological regulators such as AMPK, mTOR, insulin signaling pathways, circadian rhythms, mitochondrial function, and stress hormones are frequently treated as advanced or optional topics. Yet these mechanisms determine whether a hypocaloric diet leads to fat loss or metabolic slowdown.
Without this biological foundation, learners may apply dietary interventions correctly on paper but fail to anticipate physiological resistance. Obesity then appears “stubborn” or “non-compliant,” when in reality the biology was never addressed.
Why Functional Nutrition Reorders Obesity Education
Functional nutrition does not simply offer alternative interventions; it changes the order in which obesity is taught.
Instead of starting with weight, it starts with regulation. Instead of focusing on restriction, it examines signaling. Instead of asking “How do we reduce calories?”, it asks “Why is the body defending energy storage?”
From a learner’s perspective, this reordering is transformative. Obesity is no longer framed as a failure of discipline but as a logical biological response to chronic stress, metabolic overload, hormonal disruption, circadian misalignment, and inflammatory signaling.
This is why functional nutrition education often feels like an upgrade rather than a contradiction to prior learning. It fills the gaps traditional education leaves behind.
What Practitioners Are Forced to Unlearn
Many practitioners reach a point where they realize that obesity education has trained them to blame outcomes instead of understanding processes.
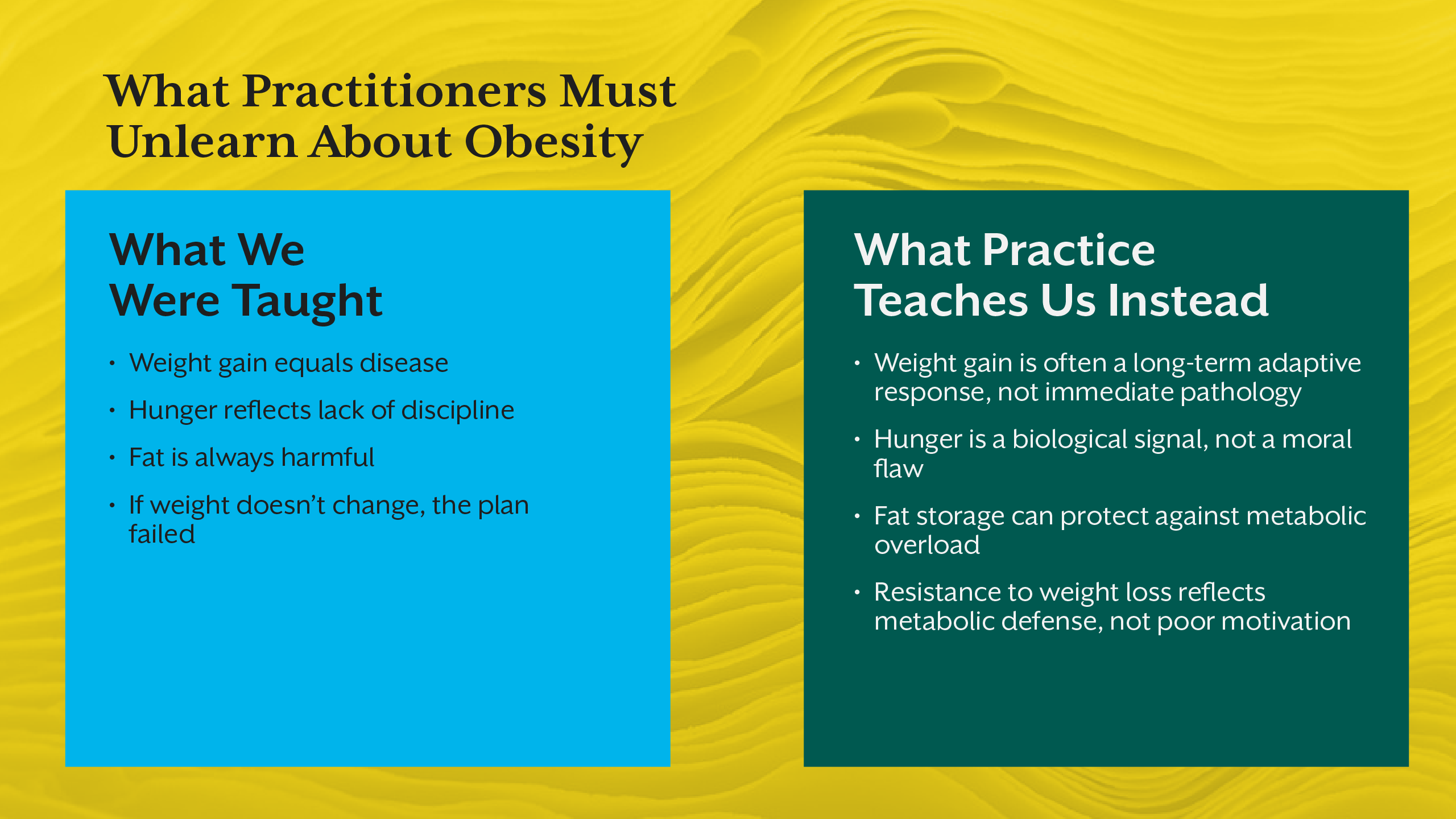
Unlearning becomes necessary:
- Weight gain is not immediate pathology.
- Hunger is not moral failure.
- Fat storage can be protective.
- Resistance to weight loss often reflects metabolic defense, not poor motivation.
This unlearning phase is uncomfortable but essential. It is also where many practitioners begin seeking advanced education that aligns better with real-world complexity and long-term outcomes.
The Cost of Teaching Obesity Wrong
When obesity is taught incorrectly, the consequences extend beyond individual learners. Practitioners experience frustration and burnout. Clients internalize blame. Interventions cycle repeatedly without durable results.
At a systems level, miseducation perpetuates stigma, oversimplified public health messaging, and ineffective care models. Correcting how obesity is taught is not an academic exercise; it is a clinical and societal necessity.
Rebuilding Obesity Education for the Next Generation
Obesity education must evolve to reflect what science already shows. This means teaching timelines, compensation, systems communication, and metabolic resilience alongside dietary strategies.
Academy-level education, such as iThrive Academy’s advanced learning pathways and iThrive Certified Functional Nutrition (ICFN) program, aim to bridge this gap by aligning education with biological reality rather than outdated simplifications.
Key Takeaway
Obesity is not poorly understood because science is lacking, it is misunderstood because education is misaligned. Traditional nutrition education often teaches obesity from the endpoint backward, overlooks compensation, fragments biology, and overemphasizes food while underteaching regulation. When obesity is reframed as a dynamic, adaptive, systems-level process, practitioners gain clarity, compassion, and clinical precision. Fixing obesity outcomes begins with fixing how obesity is taught.




.jpg)