Introduction
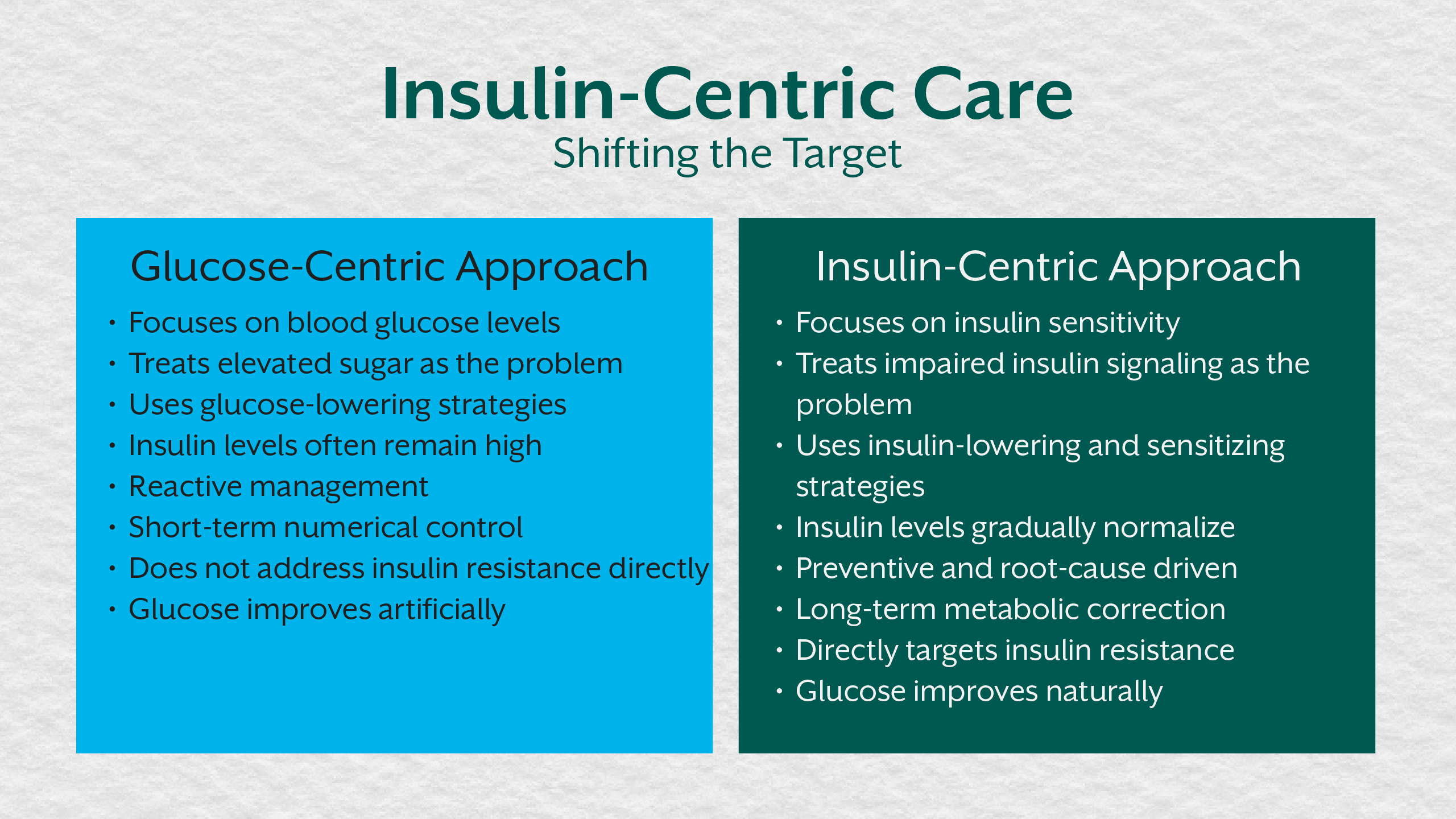
For decades, diabetes management has revolved around one central number: blood glucose. Fasting glucose, postprandial readings, and HbA1c have shaped diagnosis, treatment decisions, and patient education across healthcare systems. While these markers offer useful information, they represent late-stage outcomes, not the underlying cause of metabolic dysfunction.
Type 2 diabetes does not begin with high blood sugar. It begins with insulin resistance, rising insulin demand, impaired cellular signaling, and metabolic overload that can persist silently for years. During this phase, glucose may remain normal while insulin levels climb steadily, placing increasing strain on pancreatic beta cells and peripheral tissues.
A shift from glucose-centric care to insulin-centric thinking is not just beneficial, it is necessary. Understanding insulin resistance in diabetes reframes prevention, improves diabetes education, and allows for earlier, more effective metabolic intervention.
The Limits of Glucose-Centric Diabetes Management
Why Blood Glucose Alone Tells an Incomplete Story
Blood glucose reflects how well the body is maintaining short-term balance, not how hard it is working to do so. In early metabolic dysfunction, insulin secretion rises to compensate for declining insulin sensitivity. This compensation can preserve normal glucose levels for years.
By focusing primarily on blood glucose control, clinicians often miss the escalating insulin resistance and metabolic stress developing underneath. HbA1c rises only after pancreatic compensation begins to fail, making it a delayed indicator of disease progression rather than an early warning sign.
This glucose-first framework reinforces reactive care, where intervention begins only after metabolic damage is established.
Insulin Resistance as the Core of Type 2 Diabetes
Understanding Insulin Resistance in Diabetes
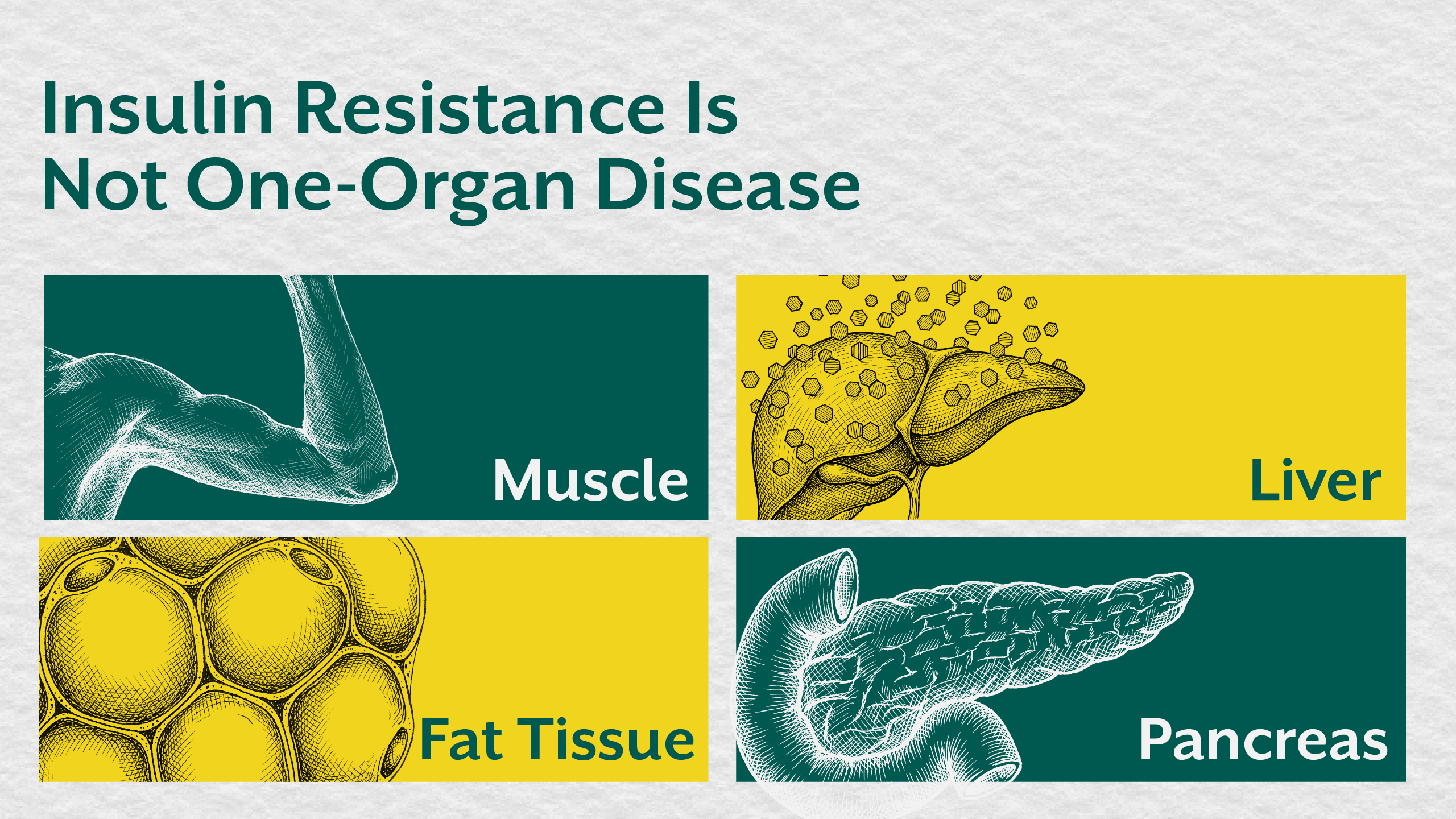
Insulin resistance occurs when cells fail to respond effectively to insulin’s signal. Skeletal muscle reduces glucose uptake, the liver continues producing glucose despite insulin presence, and adipose tissue releases excess free fatty acids and inflammatory mediators.
To maintain blood glucose control, the pancreas increases insulin output. This state of chronic hyperinsulinemia may persist long before diabetes is diagnosed, gradually worsening metabolic dysfunction.
Recognizing insulin resistance as the foundation of type 2 diabetes management shifts the focus from lowering glucose to restoring insulin sensitivity and metabolic health.
Metabolic Dysfunction Precedes Hyperglycemia
The Silent Phase of Disease
Metabolic dysfunction develops gradually through nutrient excess, physical inactivity, circadian disruption, chronic stress, and micronutrient insufficiencies. These factors impair mitochondrial efficiency and insulin signaling long before glucose abnormalities appear.
During this phase, insulin resistance increases while blood glucose remains deceptively stable. This explains why many individuals with normal glucose readings already exhibit fatigue, weight gain, inflammatory markers, and declining metabolic health.
For a deeper exploration of this early disease phase, readers may refer to the iThrive Academy blog “Insulin Resistance as a Pre-Diagnostic State: Why Type 2 Diabetes Is a Late Clinical Label.”
Why Insulin-Centric Thinking Improves Diabetes Education
Reframing Patient and Practitioner Understanding
Diabetes education that focuses solely on sugar avoidance and glucose numbers oversimplifies a complex metabolic condition. Insulin-centric thinking explains why calorie restriction alone often fails, why weight loss plateaus occur, and why symptoms persist despite “controlled” glucose values.
When patients understand insulin resistance, they gain clarity on how sleep, stress, meal timing, nutrient density, and physical activity influence metabolic health beyond blood glucose control.
This educational shift empowers sustainable behavior change rather than short-term compliance.
Clinical Implications for Type 2 Diabetes Management
Moving From Control to Correction
Insulin-centric diabetes management prioritizes reducing insulin demand and restoring metabolic flexibility. This includes addressing lifestyle stressors, improving sleep quality, optimizing nutrient intake, and correcting deficiencies that impair insulin signaling.
By intervening at the level of insulin resistance, clinicians can slow disease progression, reduce medication dependence, and improve long-term metabolic outcomes.
Why This Shift Matters for Future Metabolic Health
Population-Level Impact
With rising rates of type 2 diabetes worldwide, glucose-centric models are proving insufficient. Insulin-centric thinking offers a framework that aligns prevention, education, and intervention with biological reality.
This approach improves metabolic health outcomes not just for diagnosed patients, but also for those in pre-diagnostic stages who would otherwise remain undetected.
The Role of Education in Advancing Care
Programs that train practitioners to interpret insulin resistance markers and metabolic patterns are critical for advancing diabetes care. Educational initiatives like the iThrive Certified Functional Nutrition (ICFN) program equip health professionals with the tools to move beyond glucose-focused protocols toward systems-based metabolic assessment.
This shift is essential for improving diabetes education and long-term patient outcomes.
Key Takeaway
Type 2 diabetes is not a disorder of sugar alone. It is a condition rooted in insulin resistance, metabolic dysfunction, and prolonged compensatory stress that develops long before glucose rises. Shifting from glucose-centric care to insulin-centric thinking allows for earlier detection, more effective diabetes management, and a deeper understanding of metabolic health. By addressing insulin resistance rather than merely controlling blood glucose, clinicians and individuals alike can move from reactive disease management to proactive metabolic restoration.




.jpg)