Introduction
Diabetes risk assessment in conventional practice remains largely glucose-centric. Fasting glucose, postprandial glucose, and HbA1c are used as primary decision-making tools, often giving reassurance until values cross diagnostic thresholds. However, these markers identify late-stage metabolic dysfunction, not its origin.
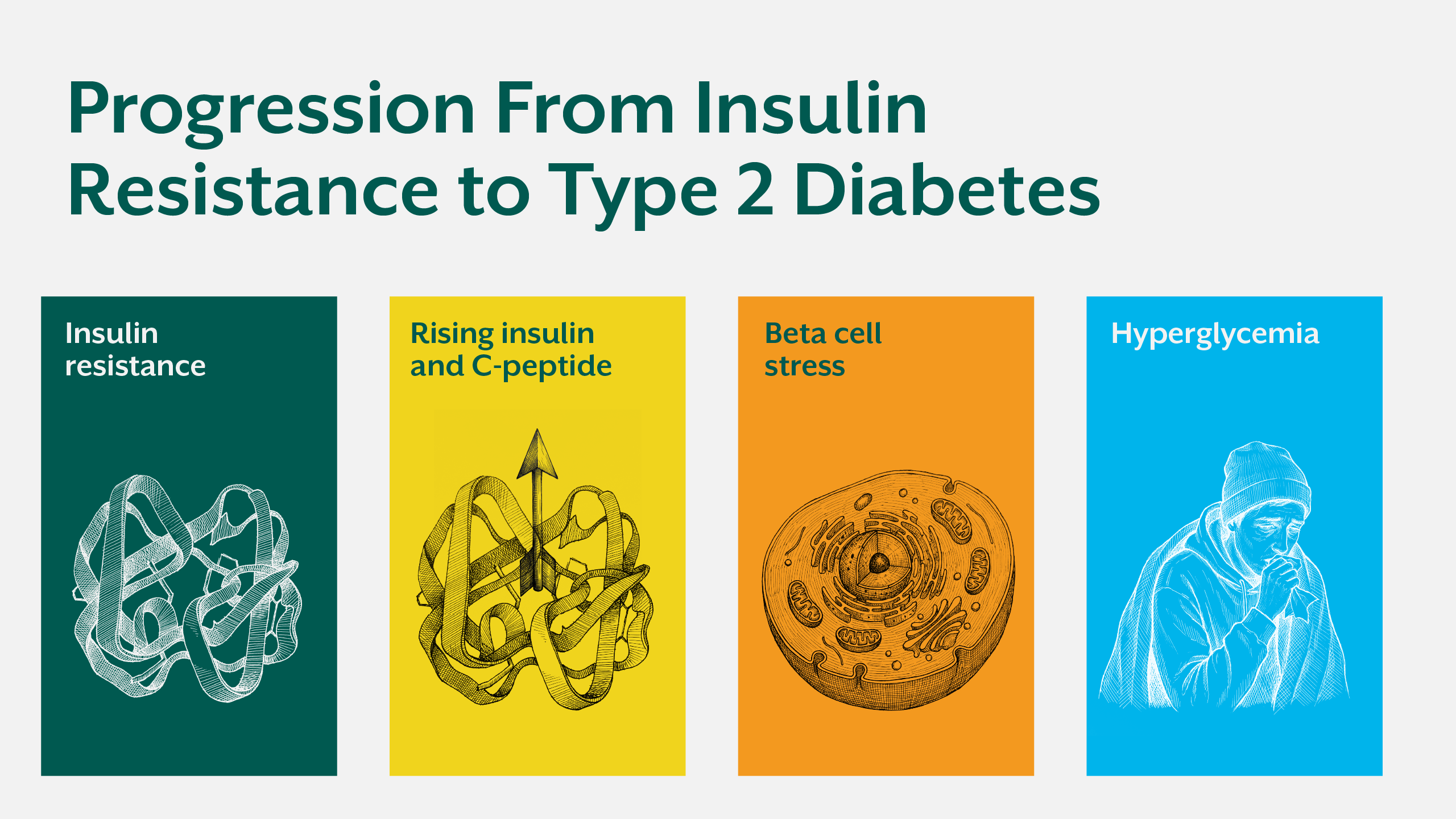
Long before glucose rises, the body enters a phase of compensatory hyperinsulinemia, progressive insulin resistance, and increasing insulin load. During this period, pancreatic beta cells work aggressively to maintain normoglycemia, masking metabolic stress that continues silently at the cellular level.
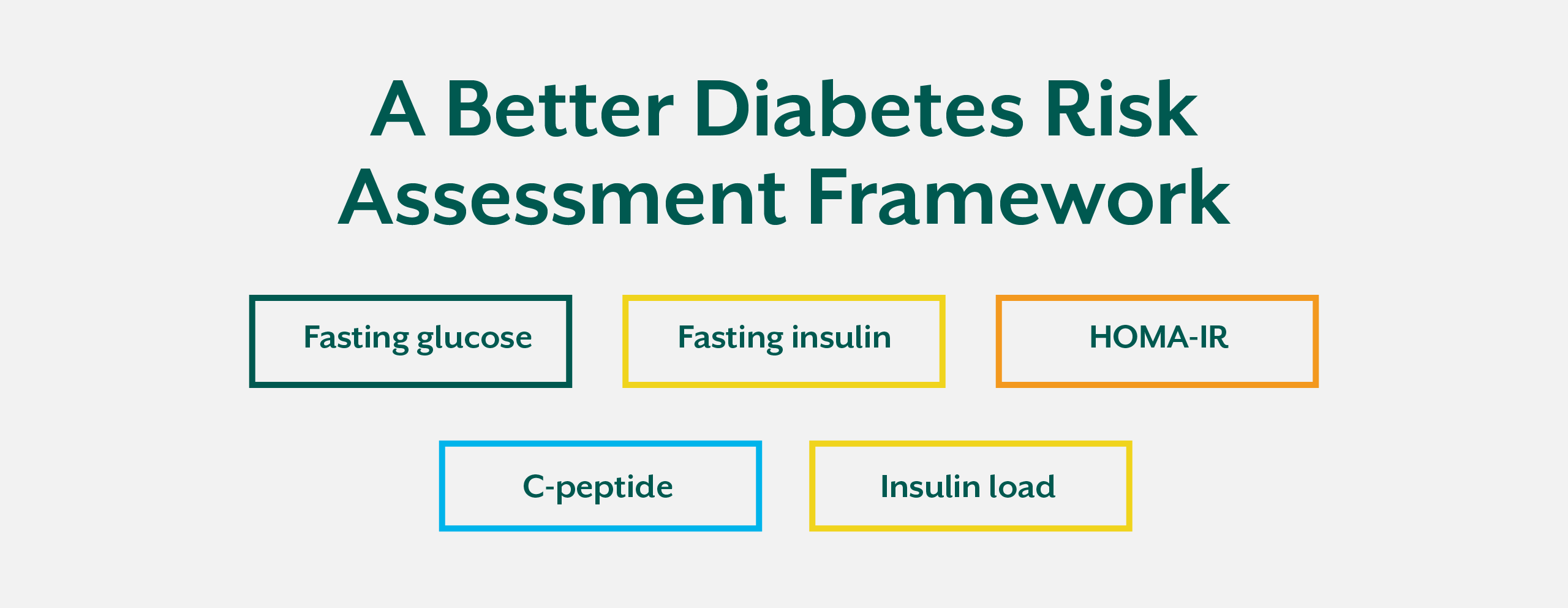
Markers such as the HOMA-IR test, fasting insulin levels, and the C-peptide test allow clinicians to identify insulin resistance far earlier than glucose-based tests. When combined with an understanding of insulin load, these tools create a more accurate and physiologically relevant framework for diabetes risk assessment.
Why Glucose-Based Screening Falls Short
The Problem With Late Markers
Glucose is tightly regulated because the body prioritizes maintaining blood sugar within a narrow range. As insulin resistance develops, the pancreas simply increases insulin output to compensate. This allows glucose to remain normal for years, even while metabolic damage accumulates.
HbA1c reflects average glucose exposure over the previous two to three months. By the time it rises, insulin resistance has often been present for a decade or more. At this stage, beta cell stress, mitochondrial dysfunction, and ectopic fat accumulation are already established.
Relying solely on glucose delays intervention and shifts clinical care toward disease management rather than prevention.
HOMA-IR: Quantifying Insulin Resistance
What Is the HOMA-IR Test?
HOMA-IR (Homeostatic Model Assessment of Insulin Resistance) is a calculated index derived from fasting insulin levels and fasting glucose. It estimates how hard the pancreas must work to maintain glucose balance.
Rather than identifying hyperglycemia, HOMA-IR insulin resistance assessment reflects insulin demand, making it a valuable early insulin resistance test.
Elevated HOMA-IR indicates that insulin sensitivity is declining, even when glucose appears normal.
Clinical Relevance of HOMA-IR
In practice, HOMA-IR helps identify individuals who are metabolically unhealthy despite normal glucose values. It allows clinicians to intervene earlier with lifestyle, nutritional, and metabolic strategies aimed at restoring insulin sensitivity.
For readers seeking deeper insight into how insulin resistance develops before diagnosis, the iThrive Academy blog “Hyperinsulinemia: The hidden driver of type 2 diabetes” provides a comprehensive foundation.
C-Peptide: Understanding Pancreatic Output
Why the C-Peptide Test Matters
C-peptide is released in equal amounts with endogenous insulin. Unlike insulin, it is not affected by hepatic clearance, making it a more stable indicator of true insulin production.
The C-peptide test helps differentiate between insulin deficiency and insulin excess. In early metabolic dysfunction, C-peptide levels are often elevated, reflecting compensatory hyperinsulinemia.
This marker is particularly useful in understanding whether elevated glucose results from beta cell failure or long-standing insulin resistance.
C-Peptide in Diabetes Risk Assessment
Elevated C-peptide alongside normal glucose indicates that the pancreas is under sustained demand. This state precedes beta cell exhaustion and rising glucose, making it a critical early marker of diabetes risk.
Insulin Load: The Missing Context
Beyond Glycemic Index
Insulin load refers to the cumulative insulin demand generated by diet, lifestyle, stress, and metabolic state. It is influenced not only by carbohydrates, but also by protein intake, meal frequency, circadian disruption, and chronic stress.
Two individuals with identical glucose readings may have vastly different insulin loads, depending on insulin sensitivity and metabolic flexibility.
Ignoring insulin load leads to underestimation of metabolic strain and missed opportunities for early intervention.

Integrating Early Insulin Resistance Markers
A Systems-Based Framework
When used together, HOMA-IR, fasting insulin levels, and C-peptide provide a layered view of metabolic health. They reveal whether glucose control is maintained through healthy insulin sensitivity or excessive pancreatic compensation.
This integrated approach allows clinicians to identify early markers of diabetes long before irreversible damage occurs.
Clinical Implications for Prevention and Practice
Early identification of insulin resistance allows for targeted interventions that reduce insulin demand and restore metabolic flexibility. These may include dietary restructuring, improved sleep, stress modulation, and correction of micronutrient deficiencies that impair insulin signaling.
Educational frameworks that train practitioners to interpret these markers are essential. Programs such as the iThrive Certified Functional Nutrition curriculum equip clinicians with the tools to move beyond glucose-centric models toward true metabolic assessment.
Reframing Diabetes Risk Assessment
Diabetes risk assessment must evolve from reactive glucose management to proactive metabolic evaluation. Insulin sensitivity tests and early insulin resistance markers provide actionable insight into disease trajectory.
When clinicians assess insulin dynamics rather than glucose alone, prevention becomes possible rather than aspirational.
Key Takeaway
HOMA-IR, C-peptide, and insulin load offer a far more accurate framework for diabetes risk assessment than glucose alone. These markers illuminate the hidden phase of metabolic dysfunction where insulin resistance and hyperinsulinemia silently progress despite normal glucose values. By identifying insulin strain early, clinicians and individuals gain the opportunity to intervene before beta cell failure and irreversible disease develop. The future of diabetes prevention lies not in chasing sugar levels, but in understanding insulin dynamics and cellular energy metabolism.




.jpg)