Introduction
If you are a practitioner, educator, or clinical learner, you’ve probably noticed something unsettling about hypertension treatment.
Patients take medication. Numbers improve.
But regulation often does not.
Blood pressure drops yet stress responses remain exaggerated.
Vascular stiffness persists.
Metabolic signalling stays impaired.
Autonomic tone remains dysregulated.
This is where pharmacology becomes intellectually uncomfortable.
Because once you move beyond prescription algorithms, a deeper question appears:
What exactly are hypertension drugs modifying and what are they not touching?
Most clinical training teaches medication classification based on drug targets: kidney, heart, blood vessels, hormones. That is useful, but incomplete. It explains where drugs act, not how they reshape regulatory physiology.
And if you are guiding patients long term or teaching future practitioners, that distinction matters enormously.
Hypertension medications do not simply lower pressure. They alter control loops:
- autonomic signalling
- vascular responsiveness
- renal volume calibration
- endocrine tone
- cellular ion handling
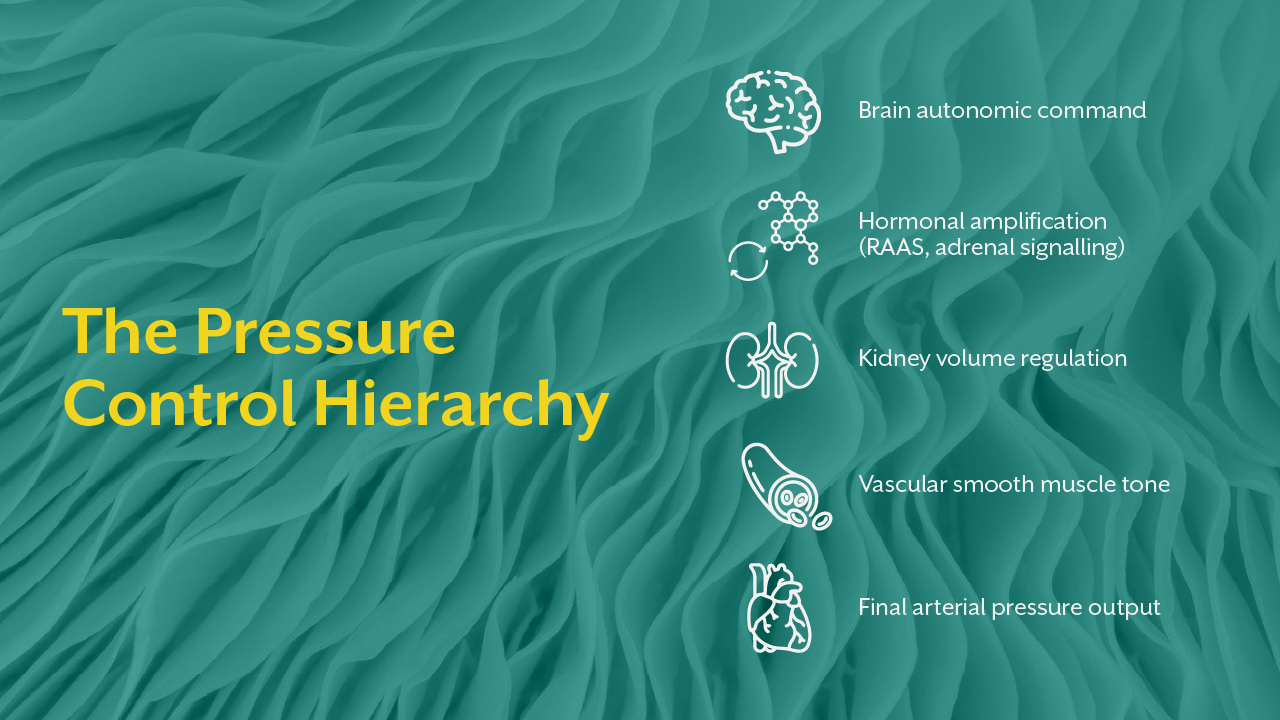
Each drug class intervenes at a different level of the pressure regulation hierarchy. Some dampen output. Some shift feedback sensitivity. Some reduce system responsiveness entirely.
Understanding hypertension drugs classification from this regulatory perspective is what transforms pharmacology from memorisation into clinical reasoning.
Today, we will examine hypertension medications not as isolated drug groups, but as modifiers of physiological control architecture.
Blood Pressure Regulation - The Targets Drugs Are Trying to Control
Before understanding hypertension drugs, you must revisit the system they attempt to influence.
Blood pressure is governed by four integrated regulatory domains:
- Neural drive (autonomic balance)
- Vascular resistance (smooth muscle tone)
- Circulatory volume (renal sodium and water handling)
- Hormonal modulation (RAAS, adrenal signalling, endothelial mediators)
Medications do not “fix hypertension.” They intervene in one or more of these control pathways to prevent pressure from rising beyond a threshold.
Think of them as regulatory dampeners.
Some reduce system sensitivity.
Some reduce output force.
Some reduce signal intensity.
Some block signal reception entirely.
When you understand this, hypertension drugs classification becomes logical rather than arbitrary.
The Nervous System as a Pharmacological Target
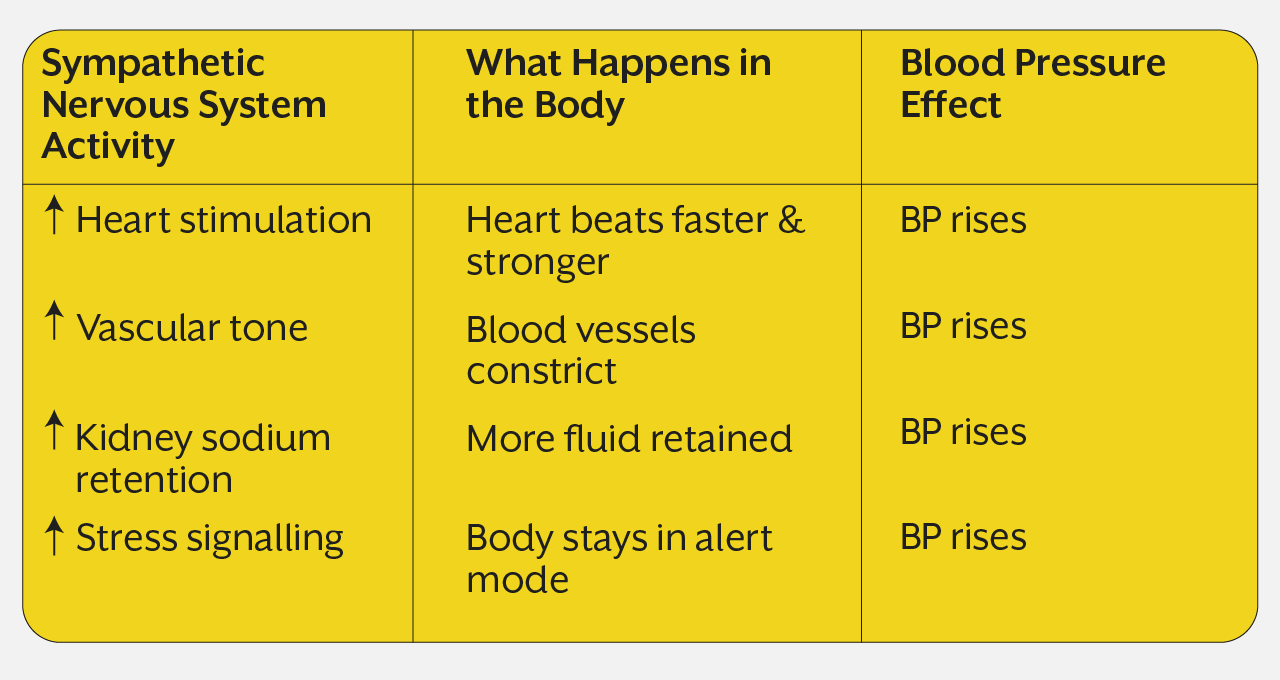
One of the most powerful and often underappreciated drivers of blood pressure is sympathetic nervous system activity.
Persistent sympathetic activation elevates vascular tone, increases cardiac output, enhances sodium retention, and amplifies stress reactivity. In many individuals, pressure elevation reflects excessive neural drive more than structural disease.
Several hypertension medications work by dampening this neural output.
Beta-adrenergic blockers
These reduce heart rate, decrease cardiac contractility, and blunt sympathetic stimulation of vascular tissue. But more importantly, they alter how strongly the cardiovascular system responds to neural signalling.
Central sympatholytics
These act within the brainstem to reduce overall sympathetic outflow. Instead of blocking peripheral effects, they lower the command signal itself.
This distinction matters clinically. Peripheral blockers reduce response. Central agents reduce generation of signal.
Understanding this difference is essential when working with patients whose blood pressure is strongly stress-reactive or autonomically labile.
The connection between autonomic regulation and cardiovascular recovery is explored deeply in the iThrive Academy article “Decoding Functional Sports Nutrition: How Electrolytes and HRV Define True Athletic Recovery.” It demonstrates how variability in neural signalling determines cardiovascular adaptability, the same principle that many hypertension drugs attempt to stabilise pharmacologically.
Renal Volume Regulation - Controlling Pressure Through Fluid Balance
If neural control sets pressure responsiveness, renal function sets baseline pressure volume.
The kidneys determine how much fluid remains within circulation. More fluid equals greater vascular filling and higher pressure potential.
Many hypertension medications target this volume control mechanism.
Diuretics
These increase sodium and water excretion, reducing plasma volume. But beyond simple fluid removal, they reset pressure-natriuresis relationships eventually altering how kidneys respond to pressure changes.
RAAS-modulating drugs
ACE inhibitors and angiotensin receptor blockers reduce angiotensin signalling, decreasing vasoconstriction and sodium retention simultaneously.
This dual action is why they are so widely used. They influence both vascular tone and volume regulation.
From a regulatory standpoint, RAAS blockers reduce the hormonal amplification loop that normally increases pressure during perceived circulatory insufficiency.
Interestingly, endocrine signalling hierarchies that influence blood pressure are also central to metabolic disease development. The iThrive Academy article “Insulin Resistance: The Silent Phase Before Type 2 Diabetes” illustrates how hormonal control systems often shift long before disease becomes clinically visible, the same anticipatory dysregulation seen in early hypertension.
Vascular Smooth Muscle - Direct Control of Resistance
Another major target in hypertension drugs classification is vascular resistance itself.
Blood vessels are not passive tubes. They actively constrict and relax in response to neural, hormonal, and local biochemical signals.
Some medications act directly on vascular smooth muscle.
Calcium channel blockers
These reduce calcium entry into smooth muscle cells, limiting contraction and promoting vasodilation.
But their deeper physiological effect is reducing vascular responsiveness. Even if constrictor signals are present, the vessel cannot contract as strongly.
This is not just dilation. It has reduced contractile capacity.
That distinction explains why these drugs are particularly effective in individuals with high peripheral resistance independent of fluid volume or neural drive.
Endothelial and Local Regulatory Modifiers
Some hypertension medications influence local biochemical mediators, the substances released directly within vascular tissue that affect tone moment to moment.
These include drugs that enhance nitric oxide availability or alter local vasodilatory signalling.
Their action is not systemic suppression but local regulatory enhancement.
They improve the vessel’s intrinsic ability to maintain appropriate tone.
This level of intervention reflects a more subtle pharmacological strategy further supporting physiological regulation rather than suppressing it.
Why Medication Response Varies Between Patients
This is where clinical reality becomes complex.
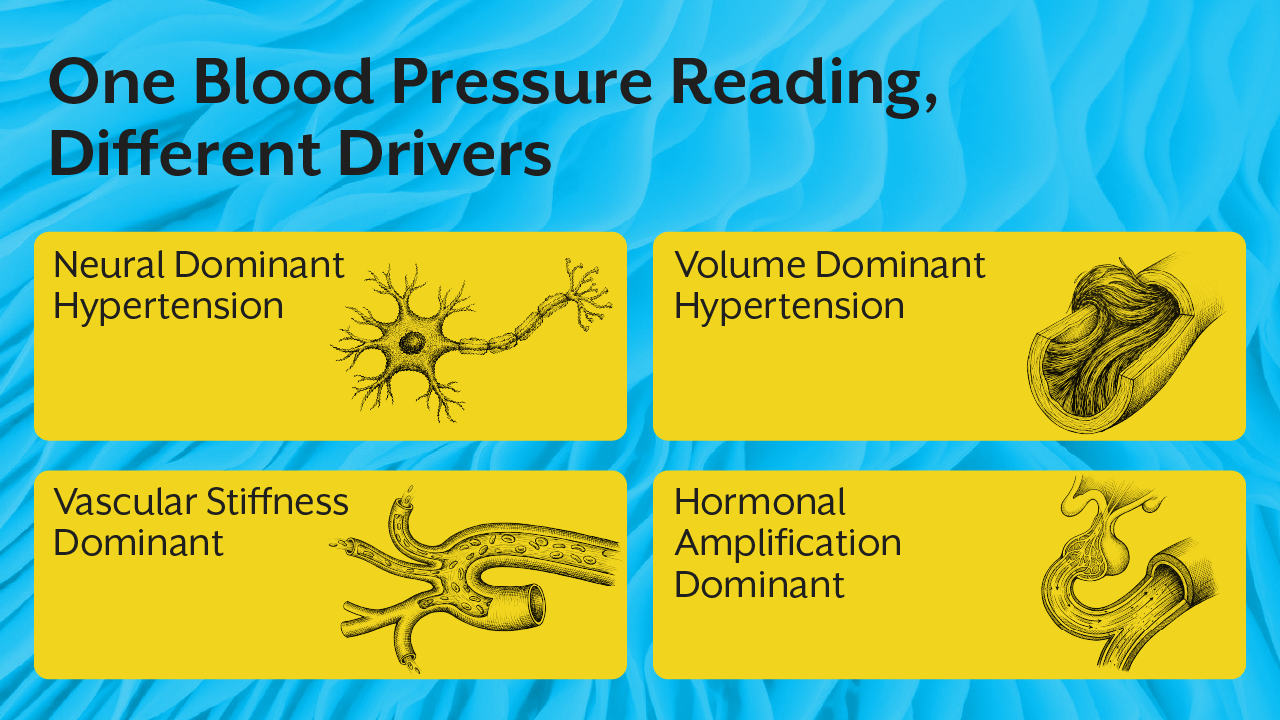
Two patients may have identical blood pressure readings yet respond completely differently to the same medication.
Why?
Because hypertension is not a single disease. It is a regulatory pattern.
One patient’s pressure may be neural-dominant.
Another’s renal-volume driven.
Another’s vascular-structural.
Another’s endocrine-amplified.
Medication effectiveness depends on matching drug mechanism to dominant regulatory drivers.
This is where systems-based clinical education becomes essential. Without understanding physiological hierarchy, treatment becomes trial-and-error rather than targeted intervention.
This integrative reasoning approach is central to practitioner training at iThrive Academy, where hypertension pharmacology is taught alongside autonomic assessment, metabolic pattern recognition, and regulatory physiology mapping, and not in isolation.
Within the iThrive Certified Functional Nutrition (ICFN) program, learners are trained to interpret medication effects within broader system behaviour, further understanding not just what a drug does, but also what regulatory imbalance requires it.
The Clinical Limitation of Drug-Centric Thinking
Here is a difficult but necessary insight.
Hypertension medications are powerful. But they do not fully restore regulatory adaptability. They stabilize output. They do not always restore dynamic control.
For example:
A drug may reduce vascular resistance but not restore endothelial responsiveness.
A drug may reduce sympathetic tone but not correct chronic stress signalling.
A drug may reduce fluid volume but not reset renal sensitivity.
This is why some patients remain physiologically unstable despite controlled numbers.
For practitioners, the critical skill is recognising when pharmacology is managing output versus restoring regulation.
That distinction shapes long-term patient strategy, education, and care planning.
Key Takeaway
Hypertension drugs classification is not simply a pharmacological taxonomy, rather it is a map of how modern medicine intervenes in human pressure regulation. Each class of hypertension medications targets a specific control pathway: neural drive, vascular resistance, fluid balance, hormonal amplification, or local endothelial signalling. But medications do not act on blood pressure in isolation; they reshape the responsiveness, sensitivity, and output of complex physiological networks.
For practitioners and clinical learners, the true mastery lies not in memorising drug names but in understanding which regulatory mechanism is dominant in a given patient and how pharmacological intervention modifies system behaviour. When hypertension drugs are understood as modifiers of control architecture rather than pressure-lowering tools, treatment becomes more precise, interpretation becomes more meaningful, and clinical reasoning moves from protocol-based to physiology-based care.




.jpg)