Introduction
If you have been trained in conventional obesity clinical education, you were likely taught structured obesity treatment protocols: calculate BMI, assess caloric intake, prescribe dietary reduction, recommend exercise, monitor weight, and escalate pharmacotherapy if required.
This framework feels systematic. It feels clinical.
Yet in practice, you may have experienced something very different.
You may have encountered patients who adhere to calorie targets but do not lose weight. Patients who experience intense hunger despite structured meal plans. Individuals who regain weight after aggressive interventions. Cases where metabolic markers worsen even when body weight decreases.
At some point, many practitioners recognize that obesity is not failing because of protocol non-compliance. It is failing because protocols alone cannot interpret biological patterns.
Teaching obesity clinically requires moving from rigid intervention frameworks to metabolic pattern recognition and understanding how signals across tissues interact over time. This is where clinical obesity management matures from algorithmic execution to systems-level reasoning.
Why Protocol-Driven Obesity Treatment Falls Short
Obesity treatment protocols are designed for standardization. They provide clarity for early learners and scalability for public health models. However, obesity is not a standardized disease state. It is an adaptive metabolic response emerging from interacting systems.
When practitioners rely exclusively on obesity treatment protocols, they often focus on:
- Caloric intake versus expenditure
- Macronutrient distribution
- BMI classification
- Stepwise medication escalation
What these models rarely teach is how to interpret:
- Hyperinsulinemia preceding weight gain
- Cortisol-driven central adiposity
- Thyroid adaptation during caloric restriction
- Leptin resistance affecting satiety signaling
- Inflammatory feedback loops from adipose tissue
Without systems biology obesity frameworks, clinical reasoning becomes reactive instead of anticipatory.
If you have ever felt that you are following every guideline yet still missing something clinically, that discomfort is not incompetence. It is the natural limitation of protocol-centered training.
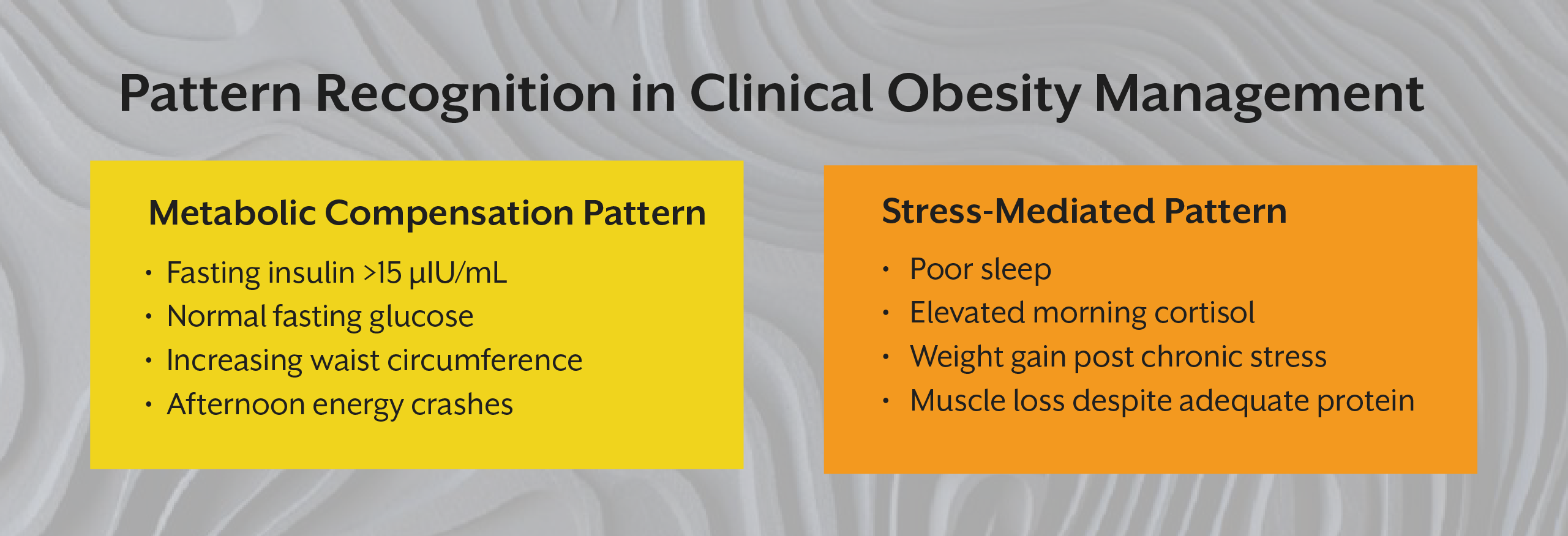
What Does Pattern Recognition Mean in Clinical Obesity Management?
Pattern recognition in obesity clinical education means identifying recurring physiological signatures across patients rather than applying the same intervention template.
For example:
A patient with:
- Fasting insulin >15 µIU/mL
- Normal fasting glucose
- Progressive waist circumference increase
- Afternoon energy crashes
- Strong carbohydrate cravings
This is not simply “overconsumption.” This is a metabolic pattern, rather compensatory hyperinsulinemia with early insulin resistance.
Another patient may present with:
- Weight gain post chronic stress
- Poor sleep
- Elevated morning cortisol
- Muscle loss despite adequate protein intake
This reflects a different metabolic signature, like stress-mediated adipose redistribution and catabolic signaling.
Teaching obesity clinically means teaching learners to ask:
- What is driving fat storage biologically?
- What is the timeline of metabolic adaptation?
- Which system initiated the cascade?
- What is compensatory versus pathological?
This shift is foundational in functional medicine obesity frameworks and is deeply aligned with systems biology obesity.
From Tissue-Based Thinking to Systems Biology Obesity
Traditional obesity education often compartmentalizes organs: adipose tissue in one module, insulin signaling in another, inflammation elsewhere. Rarely are learners trained to connect these systems dynamically.
Obesity pattern recognition requires understanding:
- Adipose tissue as an endocrine organ
- Liver as regulator of glucose flux
- Muscle as insulin sink
- Brain as appetite modulator
- Immune system as inflammatory amplifier
These systems do not fail independently. They miscommunicate.
In our previously published blog, “The Science of Obesity through a Functional Nutrition Lens,” we discussed obesity as a network-level disorder rather than a calorie imbalance. Building on that foundation, teaching obesity clinically requires translating this system's understanding into real-time clinical interpretation.
Similarly, in “What Practitioners Are Forced to Unlearn,” we explored how clinicians must release moralized narratives around weight gain. Pattern recognition expands this unlearning into technical reasoning: weight regain may be metabolic defense, not patient failure.
Teaching Obesity Clinically: A Shift in Educational Design
If you are an educator, mentor, or advanced learner, you may notice that conventional obesity clinical education teaches intervention before interpretation.
Students are taught what to prescribe before they are trained how to observe.
A clinical approach to obesity must instead prioritize:
- Timeline mapping
- Laboratory pattern clustering
- Symptom constellations
- Adaptive versus maladaptive differentiation
- Metabolic compensation tracking
For example, consider weight loss resistance. Instead of escalating restriction, pattern recognition asks:
- Is resting metabolic rate suppressed?
- Has leptin dropped significantly?
- Is T3 conversion reduced?
- Is chronic inflammation present?
- Is sleep fragmentation affecting ghrelin?
When learners are trained this way, they move from reaction to prediction.
This is where obesity clinical education evolves from protocol memorization to clinical reasoning. At iThrive Academy, particularly within the iThrive Certified Functional Nutrition (ICFN) framework, this layered interpretation becomes central to practitioner development.

Why Practitioners Struggle Without Pattern Recognition
You may have experienced this scenario:
A patient loses 8 kg, then plateaus. You increase exercise intensity. Hunger rises. Sleep worsens. Cortisol elevates. Weight rebounds.
Without metabolic pattern recognition, this appears as “non-adherence.” With pattern recognition, it appears as metabolic adaptation.
Obesity treatment protocols rarely prepare practitioners for adaptive resistance. Yet adaptive resistance is predictable when energy intake drops aggressively. The body reduces thermogenesis, alters thyroid signaling, and increases hunger hormones.
Clinical obesity management must anticipate these responses. This is not about abandoning structure. It is about integrating biological intelligence into structure.
Moving Beyond Obesity Treatment Protocols
Protocols are useful entry points. But pattern recognition determines sustainability.
In functional medicine obesity models, practitioners evaluate:
- Insulin trends over time
- Postprandial glucose variability
- Lipid particle patterns
- Visceral adiposity markers
- Stress physiology
- Gut inflammatory contributors
Root cause obesity frameworks emphasize that adiposity may be:
- Protective against toxin mobilization
- A response to chronic cortisol
- Secondary to sleep apnea
- Driven by gut dysbiosis
- Influenced by environmental endocrine disruptors
Teaching obesity clinically requires preparing learners for this complexity.
The goal is not to overwhelm. It is to refine perception. When you understand patterns, interventions become precise rather than restrictive.
Key Takeaway
Teaching obesity clinically is not about discarding protocols. It is about transcending them. When you move from intervention-first thinking to metabolic pattern recognition, your clinical reasoning deepens. You begin to anticipate adaptation, differentiate compensation from pathology, and design sustainable strategies rather than reactive adjustments. Clinical obesity management becomes less about controlling weight and more about restoring communication across systems. As a practitioner or learner, this shift is what transforms your confidence, and not because you know more guidelines, but because you understand physiology more deeply.




.jpg)