Introduction
If you’ve ever felt that thyroid education trains you to follow steps rather than understand physiology, you are not imagining it.
Most conventional thyroid training is built around simplified decision trees. Elevated TSH? Treat. Low hormone? Replace. Do symptoms persist? Adjust dose. When lab values normalize, the case is considered resolved. But real clinical practice rarely behaves this neatly.
You have likely encountered patients with persistent thyroid symptoms despite “normal thyroid levels,” unexplained fatigue even after treatment, or autoimmune patterns that fluctuate unpredictably. These are not rare clinical anomalies. They are predictable outcomes of an educational model that prioritizes protocol execution over biological reasoning.
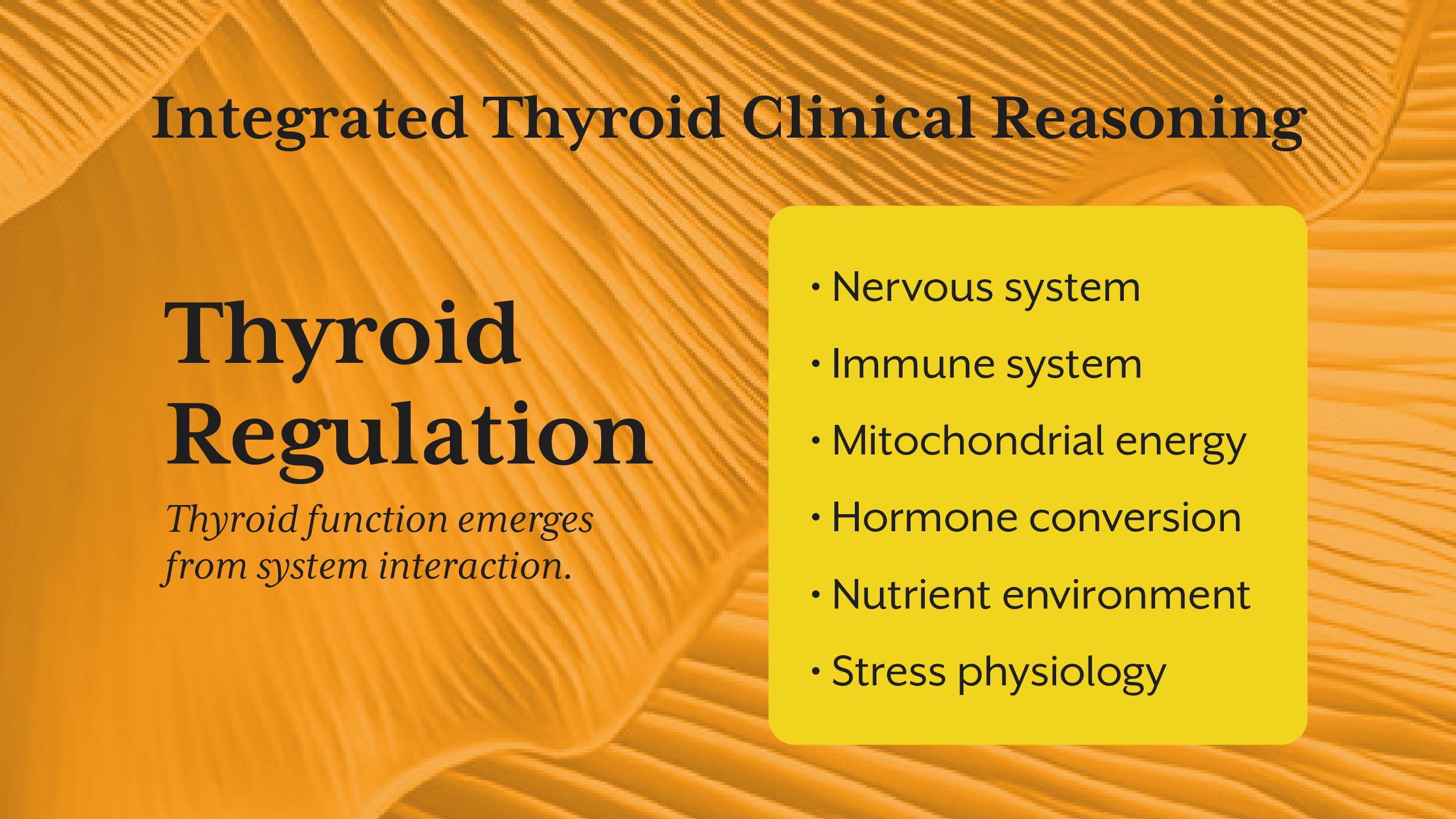
The deeper issue is not inadequate knowledge of thyroid hormone function, it is fragmented understanding of system interactions. Thyroid physiology does not operate independently. It is shaped by nervous system regulation, immune signaling, mitochondrial energy production, metabolic status, and environmental stressors. When training isolates the thyroid from these systems, practitioners learn to treat lab values rather than physiology.
This blog explores why most thyroid education produces protocol followers and what clinical thinking actually requires.
Section 1: The Reductionist Foundation of Thyroid Training
Traditional thyroid education begins with classification. Hypothyroidism, hyperthyroidism, thyroiditis, Hashimoto’s thyroiditis. Each condition is linked to a diagnostic threshold and a treatment pathway. This structure is efficient for standardization but limited for clinical reasoning.
Reductionist models assume that the thyroid gland is the primary driver of thyroid dysfunction. But in practice, many patients do not suffer from primary gland failure. They experience dysregulation in hormone conversion, immune activation, cellular responsiveness, or stress signaling.
When training focuses only on gland output, practitioners are conditioned to interpret every thyroid presentation through a narrow lens. The result is predictable, treatment decisions are based on isolated biomarkers rather than physiological context.
Clinical thinking requires pattern recognition across systems. Protocol training replaces this with categorical decision-making.
Section 2: Why Lab-Centered Thinking Limits Clinical Insight
Laboratory markers are essential tools, but they are not complete representations of physiology. Yet most training positions lab values as the definitive measure of thyroid status.
This creates a common clinical dilemma, patients with thyroid disease symptoms despite normal labs. When TSH and hormone levels fall within reference ranges, training provides little guidance. The practitioner is left with two options: dismiss symptoms or repeat testing.
The problem is conceptual. Lab values measure circulating hormone concentration, not tissue utilization. They do not reflect mitochondrial energy availability, receptor sensitivity, inflammatory interference, or autonomic nervous system influence.
Clinical reasoning begins where lab interpretation ends.
When practitioners learn to equate biochemical measurement with physiological reality, they lose the ability to investigate functional dysregulation. This is one of the primary reasons thyroid misdiagnosis occurs not because tests are inaccurate, but because interpretation is incomplete.
Section 3: The Nervous System - The Regulator Training Ignores
One of the most striking omissions in conventional thyroid education is stress physiology.
The autonomic nervous system directly influences thyroid hormone production, conversion, and cellular responsiveness. Chronic sympathetic activation can suppress peripheral conversion, alter immune signaling, and modify metabolic rate independent of hormone concentration.
Yet most thyroid curricula barely address this regulatory layer.
Understanding stress physiology transforms clinical interpretation. A patient with chronic sympathetic dominance may exhibit fatigue, weight gain, and hormonal dysregulation despite normal hormone levels. The issue is not hormone deficiency, it is regulatory suppression.
This connection becomes especially clear when viewed alongside the insights discussed in the iThrive Academy blog “The Nervous System and Obesity: Why Stress Physiology Drives Weight Gain.” The same stress-driven regulatory mechanisms that alter metabolic signaling also shape thyroid responsiveness.
When training excludes nervous system regulation, practitioners are left treating downstream effects rather than upstream drivers.

Section 4: Hormone Presence Is Not Hormone Effect
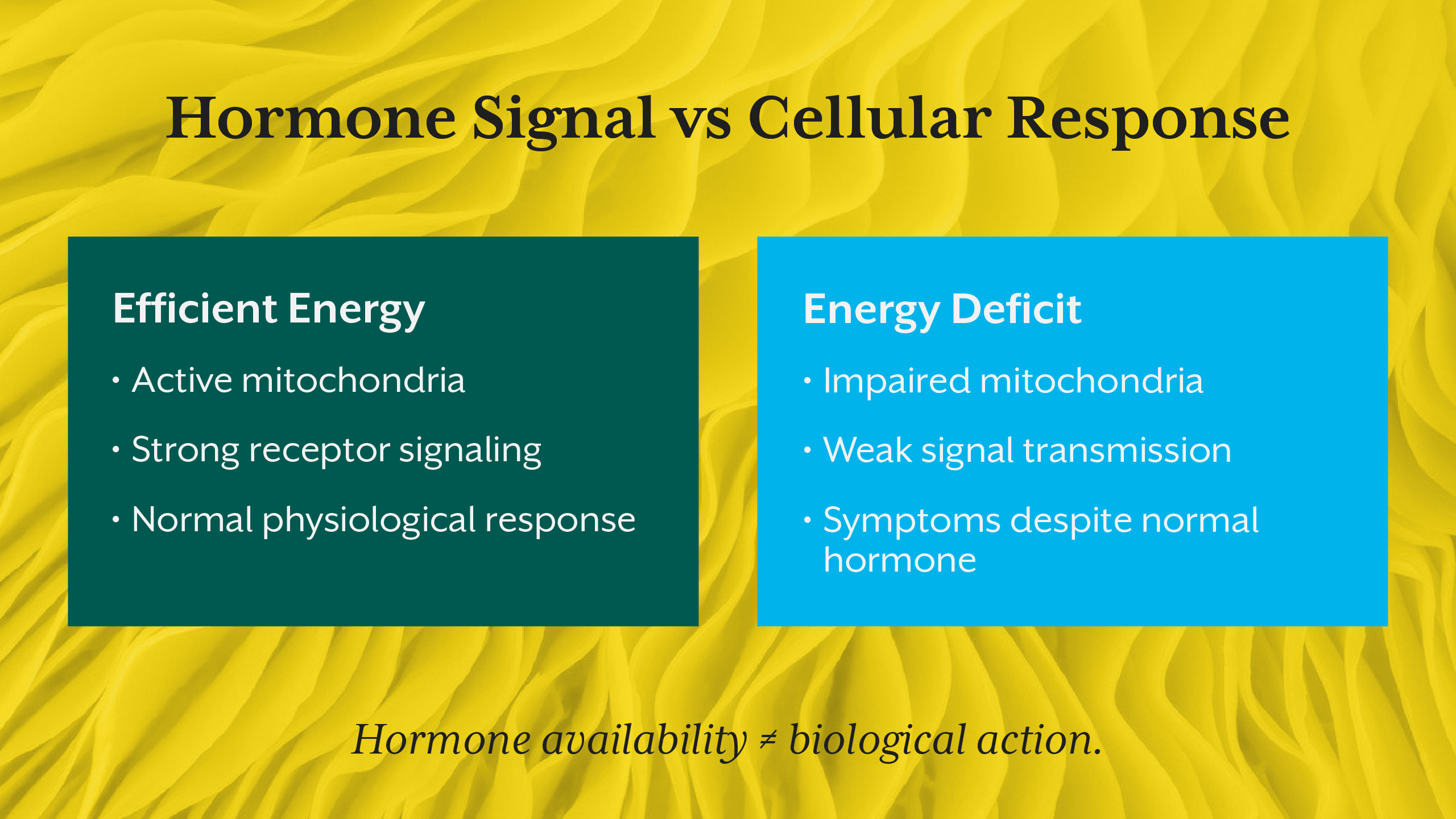
Another conceptual gap in thyroid training is the assumption that hormone availability equals biological action.
Thyroid hormones exert their effects at the cellular level, and this process depends heavily on mitochondrial energy production. Cells require adequate energy to respond to hormonal signals. When energy production is impaired, signaling weakens even when hormone levels are sufficient.
This explains why some individuals experience classic hypothyroid symptoms despite adequate circulating hormones. The signal arrives, but the cell cannot execute the response.
This principle parallels metabolic education shifts described in the iThrive Academy blog “From Protocols to Pattern Recognition: Teaching Obesity Clinically.” Just as metabolic regulation cannot be understood through calorie models alone, thyroid function cannot be understood through hormone concentration alone.
Clinical thinking requires evaluating energy dynamics, not just endocrine output.
Section 5: Autoimmune Complexity Beyond Diagnosis
Most thyroid education treats autoimmune thyroiditis primarily as a diagnostic category. Once antibodies confirm Hashimoto’s thyroiditis, the clinical process shifts toward hormone replacement.
But autoimmunity is not a static condition. It is a dynamic immune process influenced by gut integrity, inflammatory signaling, stress physiology, and environmental triggers.
Thyroid antibodies represent immune activity not merely gland destruction. Their presence reflects systemic immune dysregulation that can fluctuate over time.
Without training in immune modulation, practitioners can diagnose autoimmunity but cannot interpret its progression. They monitor outcomes rather than drivers.
This is a defining difference between protocol application and clinical reasoning.
Section 6: Why Standard Treatment Models Often Fail
When thyroid treatment focuses solely on hormone replacement, improvement depends on one assumption that hormone deficiency is the central problem.
But when dysfunction arises from impaired conversion, immune activity, stress signaling, or cellular resistance, replacement alone cannot fully restore function.
This explains why thyroid treatment sometimes fails despite normalized lab values. Treatment addressed hormone availability, but not the regulatory environment.
Clinical thinkers ask a different question: what prevents normal hormone signaling from producing normal physiological outcomes?
Protocol followers ask: what dose adjustment is needed?
Section 7: What Clinical Thinking Actually Looks Like
True clinical reasoning begins with systems integration.
Instead of asking which protocol applies, practitioners evaluate regulatory networks:
• Nervous system state
• Immune signaling patterns
• Cellular energy capacity
• Conversion efficiency
• Environmental and metabolic stressors
This perspective transforms thyroid care from linear treatment to systems assessment.
It also transforms professional identity. Practitioners shift from treatment implementers to physiological investigators.
This is the transition modern clinical education must support and why advanced learning environments such as iThrive Academy emphasize systems biology training and pattern recognition rather than isolated protocol instruction.
Key Takeaway
Most thyroid education fails not because it lacks information, but because it lacks integration. It teaches practitioners to identify disease categories and implement treatment pathways, but it does not train them to interpret physiological complexity. Thyroid function is shaped by regulatory systems like nervous, immune, metabolic, and cellular that interact continuously. When training isolates the gland from these systems, practitioners become efficient protocol users but limited clinical thinkers. True expertise emerges when hormone levels are understood within the context of energy production, immune dynamics, stress




.jpg)